In an era of widespread misinformation, it’s perhaps not surprising that people are now shirking sunscreen. Why not, eh?
Currently on TikTok, the hashtag #AntiSunscreen has amassed over 5.3 million views.
Over on X (formerly Twitter) influencer Gubba Homestead said in a video that amassed 1.2 million views: “I don’t wear sunscreen, and I never will. We blame the sun for cancer when we should be blaming our diets… Sunscreen and a poor diet will make you sick.”
Advertisement
Additionally, data from Glam reveals that this trend is having an impact on Google searches with searches for “Does sunscreen cause cancer” increasing by 160% in the past 30 days.
This is particularly frustrating as Cancer Research UK revealed this year that rates of the skin cancer melanoma — which is caused primarily by UV rays — are at the highest ever in the UK.
Alarmingly, as little as five cases of sunburn in a lifetime increase the risk of skin cancer melanoma, which can spread to other organs.
Experts urge people to apply sunscreen
This trend is not something experts approve of, or recommend.
Dr. Mariano Busso, a Beverly Hills board-certified cosmetic dermatologist, spoke with Glam and said: “Seeking health advice from content creators can be dangerous.
Advertisement
“Using sunscreen has been scientifically proven to protect skin from the harmful effects of ultraviolet light, including both UVB and UVA rays. By not using sunscreen, you are greatly increasing your odds of sun cancer.”
Studies show that regular daily use of SPF 15 sunscreen, when used as directed, can reduce your risk of developing squamous cell carcinoma (SCC) by about 40 percent, and lower your melanoma risk by 50 percent.
How often to apply sunscreen
According to John Hopkins Medicine: “Generally, sunscreen should be reapplied every two hours, especially after swimming or sweating.
“If you work indoors and sit away from windows, you may not need a second application.”
I’d listen only to experts when it comes to cancer, TBH.
TikTok Community Guidelines strictly do not allow harmful misinformation, including medical misinformation that may cause negative health effects.
At 32 years old, I was given 16 months to live. On an ordinary Tuesday morning in November, an ultrasound detected 12 lesions on my liver that would soon be confirmed as stage 4, incurable ocular melanoma.
It wasn’t supposed to happen. Just one year earlier, I had become a cancer survivor in 22 days. A single tumour was contained in my eyeball and a biopsy of the cells gave me the best possible outcome: There was a less than 2% chance of metastatic disease.
Advertisement
But somebody has to be the 2%.
My oncologist said I had one FDA-approved treatment option, and I trusted her. I didn’t have time to get a second opinion. In the 16 months she predicted I had left if I agreed to the treatment she suggested, I needed to get my affairs in order and explain to my precious nephews and niece why their (favourite) auntie wouldn’t live to see them get their drivers’ licenses, graduate or get married.
As he’d already been planning to do, my boyfriend Nick proposed to me on Thanksgiving, two days after my diagnosis. I had expected to spend the day in the corner of the room brooding over my fateful news and avoiding loved ones. His proposal and my new ring swept me up in a wave of hope and optimism for a future I wasn’t sure existed.
Courtesy of Katie Ortman Doble
The author on Thanksgiving Day in 2014, two days after her stage 4 diagnosis, as her then-boyfriend Nick proposed. “My nephew photobombed the proposal,” she writes.
And while I vacillated between planning my funeral and my wedding in my head, I had one crucial advantage in my new reality: My father is a doctor of internal medicine.
Advertisement
Before a drug becomes FDA-approved, it goes through the clinical trial process. For someone like me with an advanced, rare disease, clinical trials offered a better shot at buying more time, which is really all we’re hoping to do.
My father asked my oncologist about clinical trials.
“That would be very expensive,” was all she told us.
We, rightfully so, give doctors authority. They have advanced degrees. They dedicate their lives to understanding human biology, science and pharmaceuticals. I’m just a headhunter. What do I know?
If it were not for my father, who questioned the authority of this doctor, I would have blindly followed her. And I can say with certainty that had I done that, I would be dead right now.
Courtesy of Katie Ortman Doble
From left to right, the author’s husband Nick, the author, and her father/agent, James Ortman, get ice cream in New York City between scans and appointments at Memorial Sloan Kettering in 2015.
My father, whom I began referring to as my agent, spent every waking moment talking to doctors all over the country to find a glimmer of hope — something that could buy us more than 16 months.
Advertisement
He got me an appointment that December at Memorial Sloan Kettering in New York City. And so began my crash course in clinical trials (also called studies or protocols). My “agent,” fiancé (a word that tied me to a future in which I was alive) and I met with the doctor there, who explained our options.
He spoke about the importance of strategy in creating my treatment plan. Had I started on the first treatment option provided by the oncologist who diagnosed me, for example, I would not have been eligible for the clinical trial he was running.
Courtesy of Katie Ortman Doble
The author and Nick in 2016 when she lost her hair for the first time. “Nick and my nephew/godson Tommy both shaved their heads with me each time my hair fell out, as did my brothers, father and father-in-law,” she writes.
I have heard of other patients who frantically start chemotherapy upon a terminal diagnosis, only to find that made them ineligible for potentially life-saving clinical trials. When you’re given an expiration date, it’s hard to take a pause on attacking the thing that is attacking you, but this approach can mean having a matter of months versus years (or life and death).
All cancer treatments start as clinical trials, so clinical trials are essential in advancing medicine. The clinical trial process typically includes four phases focused on safety, efficacy, comparison to standard of care and the safety of treatment over time, and the majority of drugs fail in one of these phases. The estimated median cost to develop just one successful drug is $1 billion and approval takes 12 years on average. The FDA approval process itself takes six to 10 months.
Advertisement
The first five weeks of the MSK trial were packed with appointments, and as a Midwest girl living in Denver, I was secretly thrilled with the opportunity to temporarily live in a tiny, expensive apartment in Midtown Manhattan. While I worked in my company’s Midtown office, I also saw a Broadway show, went wedding dress shopping and found myself with a hideous, full-body rash from the trial’s side effects the week before my wedding.
Courtesy of Katie Ortman Doble
The author climbing a fourteener in Colorado through First Descents in 2016. “First Descents provides the healing power of adventure to young adults impacted by cancer and MS,” she writes. “I was the recipient of First Descents’ Out Living It Award in 2021.”
I was starting to understand the expense of clinical trials that my first doctor referenced. For me, the financial burden came from the airfare and lodging. I’ve been lucky to have excellent insurance through work and a job that allows me the time off. I have peers who have survived cancer only to be left six figures in debt, which leads to crippling stress, which in turn damages their health.
Those who don’t have insurance, or have astronomical deductibles, or can’t afford the financial demands that come with participating in a trial, aren’t able to get treatment that could save their lives. It isn’t fair that our health care system favours the privileged.
I spent eight months in treatment at MSK, flying to NYC monthly from Denver to pick up my medication and get scans. But by August of that year, the growth of my tumours eliminated me from the trial. Thankfully, we were ready with the next trial option.
Advertisement
This was another critical strategy introduced by my doctor at MSK that I encourage other patients to explore and understand. For someone like me, it wasn’t likely that I’d only do one clinical trial. While my doctor kept my tumours at bay, he and my dad continued conversations with doctors all over the country to be sure we had a plan B and C, in case I wasn’t eligible for plan B. We didn’t want to wait until I was eliminated from my first trial. We wanted to be ready. And since some trials and treatments might make me ineligible for others in the future, we had to be very methodical with our next step.
I participated in two trials back home in Denver over the next two years while also exploring Y90 or liver embolisation, something that was only FDA-approved for metastatic colon cancer at the time. My tumours responded really well to that therapy, buying me 3.5 years of stability and the chance to finally enjoy a delayed honeymoon with my husband.
Courtesy of Katie Ortman Doble
The author visiting her “happy place,” the Cliffs of Moher in Ireland, with Nick in 2016 after her third clinical trial.
In May 2020, substantial growth in my tumours pushed me into my fourth clinical trial at UPMC-Pittsburgh. Getting into clinical trials isn’t guaranteed or easy, especially when cross-country travel is involved. It typically includes a battery of tests like an EKG, echocardiogram and a CT scan or MRI. In my case, I had three liver biopsies in short order from three separate hospitals because each wanted its own tissue.
Liver biopsies feel like someone is taking a staple gun to your liver. Our bodies endure so much simply staving off cancer, not to mention the pokes and prods that come from treatment. The doctor also needs to see that you and your bloodwork are within the safety parameters of the trial.
Advertisement
Just as getting in isn’t guaranteed or easy, neither is staying in the trial. When you get eliminated from a trial, it’s usually for tumour growth or something else entirely out of your control. I was unknowingly kicked out of my second trial after one infusion because I was taking steroids that the doctor prescribed to combat one of the side effects. I was grateful that I continued to have options, but the volatility of it all was exhausting. The worst part was always the in between, when I didn’t have a plan and the fear of the next treatment haunted me.
In Pittsburgh, the goal of the TIL therapy was to re-sculpt my immune system with cancer-fighting cells. Enrolling was labour-intensive. There were the standard exams that deemed me eligible, plus the steps involved to create my treatment. The doctor laparoscopically removed two tumours from my liver and from those cells, grew the TIL or Tumour Infiltrating Lymphocytes. A leukapheresis extracted my white blood cells, which were then fed to the TIL, multiplying them from the millions to the billions.
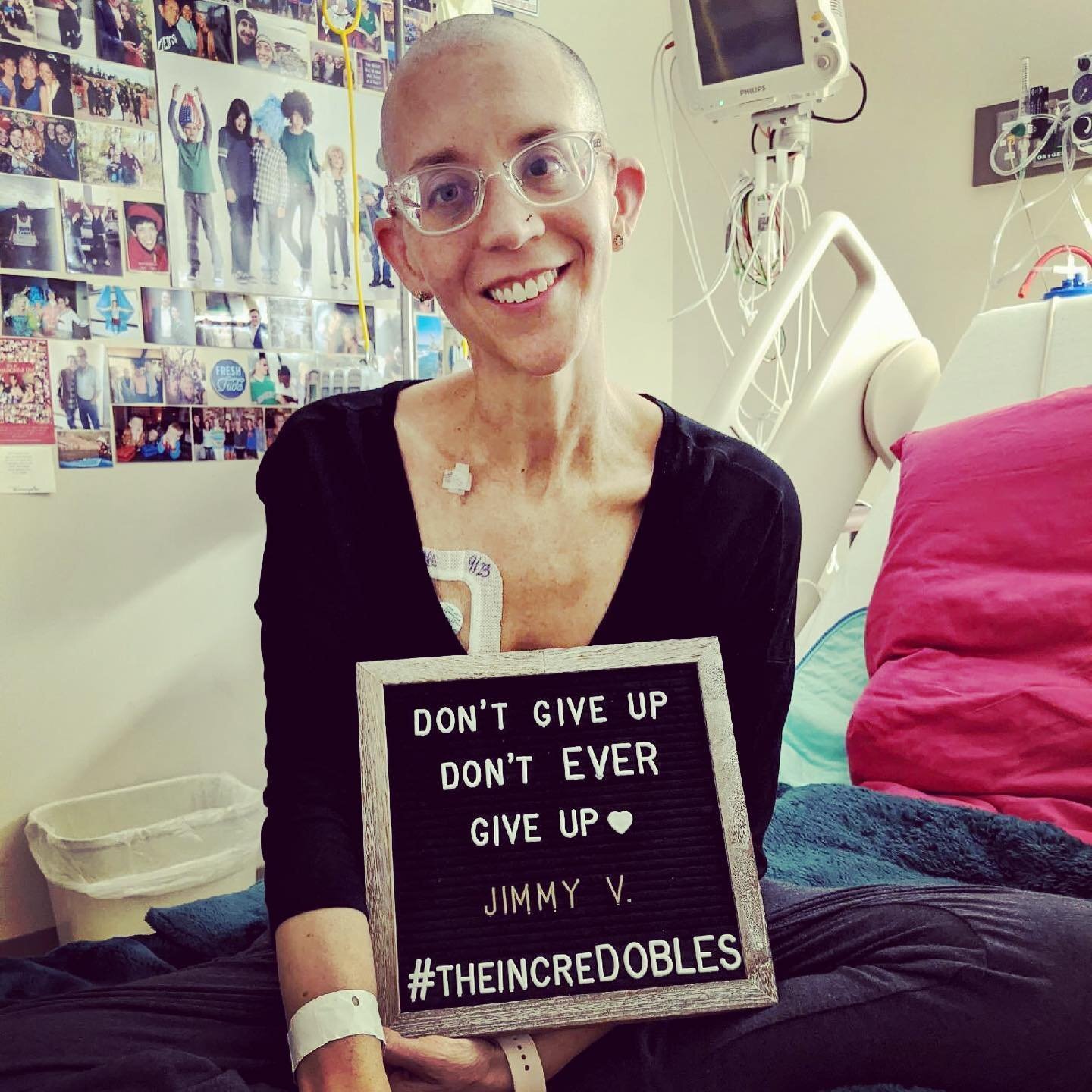
Courtesy of Katie Ortman Doble
The author in her hospital room at the end of her TIL treatment in 2020. “Nick and I branded ourselves as theincreDOBLES,” she writes.
That September, I spent three weeks in the hospital receiving seven days of chemotherapy, my TIL infusion and IL-2. Because of that one time I was unexpectedly eliminated from a trial, I held my breath until the TIL hit my bloodstream. I closed my eyes and pictured the reprogrammed cells reuniting with their former tumour friends to now attack them.
I decorated the muted coloured walls of my hospital room like a dorm with my “F*CK cancer” cross-stitch, pictures of my nephews, nieces and loved ones, and pictures of my body doing adventurous things like skydiving, kayaking and jumping into the Adriatic Sea. When my hair started to fall out, Nick shaved my head and went back to the hotel to shave his own.
Advertisement
My life started to feel like a game of whack-a-mole. But I was so grateful. Through all the flying back and forth, different doctors and side effects, I was buying time I wouldn’t have had if I’d listened to my first oncologist. At the time of my diagnosis, there was only a half page of trials to explore. When I had growth in 2020, there were over three pages.
Courtesy of Katie Ortman Doble
The author with Nick and their “doghter” Alice in 2021 after the author was told she had “no evidence of disease” (NED).
I responded well to TIL, with some tumours shrinking and a few disappearing. One rogue tumour that my doctor called the “festering problem” kept growing. Naturally, I named it Uncle Fester. In September of 2021, my doctor told me he wanted to surgically remove Uncle Fester and all remaining cancer, and I eagerly obliged.
On Sept. 17, 2021, nearly seven years after I’d been given 16 months to live, I awoke from surgery to hear the words we once thought impossible: “We got it all, Katie. You are no evidence of disease (NED).”
If it weren’t for my father/agent, I wouldn’t have known how to navigate the world of clinical trials that ultimately bought me enough time to (so far) see the first of nine nephews and nieces drive his car.
Advertisement
Clinical trials are not going to be the answer for every diagnosis, but they need to be a consideration, not an afterthought. If you or a loved one gets diagnosed with cancer, talk to your doctor about what clinical trials are available. This might require getting a second opinion — which ideally is done prior to starting any treatment.
Courtesy of Katie Ortman Doble
The author and Nick in New Zealand in 2022 celebrating her NED status.
This month marks 20 months since I became NED. My doctor continues to monitor me, and I am cautiously hopeful. Of course, there’s the chance my cancer returns. My doctor hopes that the TIL in my bloodstream remains dormant in my lymph nodes and reactivates if that happens.
I haven’t had a reason to speak to my original oncologist since seeking a second opinion, but I’m almost certain she thinks I’m dead.
Katie Ortman Doble is a headhunter, stage 4 cancer survivor, patient advocate, keynote speaker and author (blog: Future Happy Self) who is currently seeking an agent for her memoir. In 2017, Katie was given the Courage Award from the Melanoma Research Foundation. She received the First Descents′ Out Living It Award in 2021 and was recently highlighted as a Medical Hero by CISCRP. She and her husband, Nick, reside in Denver with their doghter, Alice. Connect on Liinks and follow Katie’s story of survival on Instagram/Twitter @ceortman.
Every morning I apply sunscreen, always to my face and usually to any other exposed skin too. Vanity drives my habit more than fear of skin cancer, but that vanity is going far to keeping my skin healthy — especially as a Florida resident.
But the same can’t be said for my husband.
Despite having a partner who writes about skincare and speaks enthusiastically about sunscreen, he doesn’t wear it daily.
Advertisement
But he, along with other men, have good reason to start: males are significantly more likely than females to die of melanoma, according to recent data from the US Centers for Disease Control and Prevention data. Among white people, who experience much higher rates of melanoma than people with other skin tones, males died of the cancer at more than twice the rate of females.
Lian Mack, a board-certified dermatologist and the medical director and owner of Gramercy Laser and Medical Dermatology, sees a disparity firsthand in her offices. “The number of women presenting to our offices for skin checks far exceeds the number of male patients,” she says, noting females in their mid-20s to late 50s make up the predominant demographic.
This same pattern is repeated elsewhere too. “Men seem to need a lot more coaxing to be seen in the office for skin checks,” says Luke Maxfield, a board-certified dermatologist. “Every year I have at least two or three men who are dragged into the office by their spouses only to have me confirm the diagnosis of melanoma. Literally, spouses often save men’s lives,” he says.
Advertisement
Delaying skin checks or forgoing them altogether means that problematic moles or spots may not be caught until later stages when melanoma’s survival rate begins to decrease, which can explain some of the increase in death rates. While skin cancer is more common in light skin, delaying skin checks is problematic for people of colour. Those with darker skin who are diagnosed with skin cancer often have a worse prognosis because it’s caught at a later stage.
Forgoing skin checks isn’t the only factor. Behaviour, lifestyle and even the locations of cancerous lesions make a difference.
“Women are more likely to wear sunscreen, more likely to stay out of the sun, and young women are more likely to have done a self-examination looking for skin cancers and also much more likely see a doctor for anything concerning,” Maxfield says. “These tendencies are extremely important given that more than half of melanomas may be first noticed by people examining their own skin at home.”
Without proper self-examination, those concerning spots can be hard to find and treat, especially in hard-to-see areas. “In males, most melanomas occur in areas that they are unable to monitor, like the shoulders or the back,” Mack explains, and without a partner to point it out, major delays in treatment can occur.
There may be biological factors, as well. Even when comparing melanomas of similar thickness and location between men and women, the men still fared worse. Levels of testosterone may play a role, but the science is still out on why exactly this is. “The story seems much more than just hormones, and there seems to be a biological role we have yet to discover,” he says.
Given the science, why aren’t more men wearing sun cream? When used properly, it has been proven to reduce the risk of both melanomas and other types of skin cancer. But while many people may apply sun cream when heading out to a day at the beach, making it a daily habit is essential since UV exposure is cumulative over time. “Most of my male patients need to be educated on the importance of sunscreen and the role that its use plays in the prevention of skin cancer and early aging. Most men simply do not believe that they need sunscreen if it is cold out or overcast,” Mack says.
Advertisement
It’s also not the easiest product to work with. Some sun creams can leave behind an uncomfortable stickiness or a white cast on the skin. “My skin-of-colour patients often struggle with the cosmetic elegance of sunscreen,” Mack says, explaining that some can leave behind a greyish-blue tone.
Since the effects of UV radiation damage don’t show up right away, it can be hard to connect time in the sun to any serious effects. And unlike women who use sunscreen to prevent premature ageing, men often don’t share the same motivation, Mack explains.
Making sunscreen a daily habit – even if it’s cloudy – comes down to just one thing: choosing a sun cream and applying it. “The best sunscreen is the one you use,” Mack says, repeating a quote oft-given by dermatologists.
Moyo Studio via Getty Images
For face, a cream sun cream of SPF 30 or higher is ideal, applied daily after cleansing and moisturising (skipping moisturiser is OK if it’s not needed). Applying enough is important to get full coverage – Mack recommends the two-finger method. Apply a streak of cream to two fingers from base to tip, and apply generously. “I tell my patients to put some of that product on their ears and neck as well,” Mack says.
Advertisement
Don’t forget to apply sun cream to the body, especially if you’ll be in the sun during the day. “If you are going to be at the beach and applying cream to your body, you should apply at least 2 ounces (or the size of a shot glass) to the entire body 20 minutes before sun exposure and reapply every 80 minutes,” Mack says.
Think about your lifestyle when choosing a sun cream. “Moisturisers with SPF do double-duty to hydrate and protect the skin while also providing sun protection. Tinted sun creams can help them blend with darker skin tones as well as protect from visible light and protect skin from dark spots. And if you are an active person, make sure you are getting something water-resistant,” Maxfield says.
There is good news: despite bleaker statistics for men, knowledge and prevention can go a long way. “Take control of what you can,” Maxfield says. “Know your risk factors. These include sun exposure, having multiple moles on your body, or a family history of melanoma,” he says.
Aside from seeing a dermatologist, self skin checks can be lifesaving. “Check yourself for moles that have multiple colours or irregular borders, those larger than a pencil eraser, or any changing moles, and make sure you seek out a dermatologist if there is anything concerning,” Maxfield says.