New screen time limits have been revealed for children in the UK under five.
The guidance, from the UK government, comes as almost one-quarter (24%) of parents of three‑ to five‑year‑olds say they find it hard to control their child’s screen time, and 98% of two‑year‑olds watch screens every day.
In response to parents calling for support on how much screen time is too much, as well as how to build healthy habits, the government shared new evidence-informed guidance for babies, toddlers and pre-schoolers.
Advertisement
What are the new screen time rules?
Under twos should avoid screen time other than for shared activities that encourage bonding, interaction and conversation (ie. FaceTiming family), per the new guidance.
Meanwhile two- to five-year-olds should stick to no more than one hour of screen time a day.
The government also advises avoiding screen time at mealtimes and in the hour before bed, so as not to disrupt sleep.
What else does the guidance say?
Opt for slow-paced, age-appropriate content.
Fast-paced, social media-style videos and AI toys or tools should be avoided for young children.
Parents are encouraged to watch or use screens together to make the experience more interactive, as talking, asking questions, and engaging with the content is better for children’s development.
Make safe screen swaps like reading bedtime stories together or playing simple games at mealtimes.
The guidance stems from the findings of an expert panel led by the Children’s Commissioner Dame Rachel de Souza and Professor Russell Viner, a paediatrician and expert in children’s health.
The panel reviewed the latest evidence on screen use in under-5s, and found long periods of time spent on screens alone can get in the way of activities critical for development.
Think: sleep, physical activity, creative play, and interaction with parents.
But not all screen use is equal.
Watching screens with an engaged adult where parents talk and ask questions is linked to better cognitive development than solo use.
Advertisement
Slow-paced content is also far better for development than fast-paced social media-style videos.
Evidence also suggests time limits shouldn’t apply in the same way for screen-based assistive technologies to support children with special educational needs and disabilities.
Prime minister Keir Starmer said: “Parenting in a digital world can feel relentless. Screens are everywhere, and the advice is often conflicting.”
The new guidance “cuts through the noise”, he added, “to keep children safe and make sure healthy habits are baked in from the start”.
Advertisement
Admitting that some will oppose the guidance, he added, “I will always stand on the side of parents doing their best for their children”.
Children’s Commissioner Dame Rachel de Souza said: “Young children need their parents to be confident in managing their screen use, but often this can be overwhelming for parents learning to navigate this.
“My hope is that this guidance helps to cut through the conflicting advice available and prioritise children’s development and wellbeing, as well as their safety.”
Advertisement
Neil Leitch, CEO of the Early Years Alliance, welcomed the new guidance and its emphasis on providing practical tips and advice for parents and carers.
He added he hopes it’s “the first step towards equipping children – and those supporting them – with the skills they need to thrive in an increasingly digital world and ensuring that technology enhances rather than undermines early learning and wellbeing”.
Having been there twice, I think it’s fair to say giving birth isn’t exactly a fun experience. But boy am I glad I gave birth in the 2020s and not the 1800s.
That’s for a plethora of reasons, but mainly this one…
Back in the late 1700s, doctors created a hand-operated medical instrument for cutting through bone. They discovered they could use it to help women give birth if their baby became stuck.
Advertisement
Over time, that instrument has undergone a few modifications but we now know it as the humble chainsaw.
So, the chainsaw was invented to aid with birth?
Partly, yes! As BBC Science Focus explained, the saw “was used to cut away flesh, cartilage, and bone from the mother during childbirth if the baby became stuck in the birth canal”.
Back then the saw, which became known as the “osteotome”, wasn’t like the electric chainsaws of modern day – rather, it resembled a plate with a sharp toothed chain wrapped around it, which was powered by a handle surgeons had to manoeuvre themselves. Check out this TikTok video which shows it in action.
Advertisement
It was also used in other surgeries where bone needed to be cut – such as amputations.
The tool was pretty revolutionary for doctors. According to a paper published in the journal Heritage, the osteotome helped mechanise medical procedures as prior to its invention, surgery was conducted with “hand tools, including hammers, chisels, and saws”.
Bone is notoriously pretty strong, so cutting it or trying to chisel it away with hand tools could result in “patient injury, extreme discomfort, haemorrhaging, and complications during surgery”.
Wait, but what about C-sections?
Caesarean sections (C-sections) have been occurring since the 1800s, and probably even well before then – however, historically the surgery was extremely dangerous and both mother and baby were likely to die, either from the surgery itself, shock or a post-operative infection.
Advertisement
Because of this, C-sections were often considered a last resort.
Per Pharmacy Times, the surgical procedure of the symphysiotomy was more common: “During this procedure, the pubic symphysis, which is a joint above the vulva covered and connected by cartilage and reinforced by ligaments and tendons, is severed to widen the pelvis and make the childbirth process a bit more likely to occur.”
But thanks to modern knowledge around post-operative infections as well as the advancement of anaesthesia, C-sections have gradually become more and more popular and are no longer a last resort for many expectant parents.
In England, 42% of babies were delivered by C-section between 2023 and 2024, NHS data shows.
When did chainsaws become a gardening tool?
As for the evolution of the chainsaw, in the early 1900s, people began to realise the hand-powered surgical saws could be used for other applications, too – like cutting trees.
Advertisement
So, in 1918, James Shand created and patented a portable chainsaw and in 1926, Andreas Stihl – yes, of Stihl power tools fame – developed and patented an electric chainsaw for cutting wood.
“I want you to squeeze 30%, then 60% and then 90% when I tell you to, OK?” said the physiotherapist, referring to my pelvic floor muscles.
“OK,” I replied, feeling a little overwhelmed. I’d walked into this appointment completely unsure of whether I knew how to do a kegel properly. Thankfully, we swiftly established that I could.
Advertisement
I focused as hard as I could and slowly, carefully clenched my pelvic floor muscles. I squeezed a little, then some more, and then as much as possible.
“Good,” said physiotherapist Maria Elliott. She then proceeded to tell me I was doing it properly, and my muscles were working well, but the muscle was weaker at the back than at the front.
This, she explained, is likely why I’m having occasional trouble with bladder control.
Don’t get me wrong, I can (usually) cough and sneeze and not have any problems. But ever since having two kids, if I’m physically sick, the evacuation of my stomach is usually accompanied by an evacuation of my bladder. Not ideal.
Advertisement
Maria Elliott founded The Mummy MOT in 2015. The specialist postnatal examination, for those who’ve had either vaginal or C-section deliveries, assesses how posture, pelvic floor muscles, and stomach muscles are recovering after childbirth.
The physiotherapist has since gone on to train around 900 practitioners so they can deliver the same service to new parents across the UK.
While I was lucky enough to attend a session with Maria for free for the purpose of understanding how they work, in central London, an hour-long consultation costs around £150 (the same price as a cut and colour at the hairdresser’s), while follow up sessions can be £200 each.
Advertisement
During pregnancy, it’s normal to attend multiple antenatal appointments (roughly seven to 10 depending on whether it’s your first baby or not), but once that baby is born, new mums can often feel like they’re left in the lurch.
Bar a few midwife and health visitor check-ups in the weeks after birth (usually focusing on your baby), a GP appointment at 6-8 weeks postpartum is pretty much all you get – and even that is tacked onto the baby check-up, so if the appointment runs over, you’re left with approximately five minutes to explain where your head, and body, is at.
And let’s face it, at almost eight weeks postpartum, you’re still very much healing and trying to figure out how you feel in your body and mind, all while existing on very little sleep.
Advertisement
I wasn’t really aware of any issues with my pelvic floor at eight weeks postpartum after my second child. It was only months later, when I caught a stomach bug, that I realised it wasn’t working like it should.
Around the same time I started noticing that if my bladder was fuller than usual, the odd sneeze would wreak havoc, too. Now I realise why a relative of mine always crosses her legs when she sneezes.
But we shouldn’t have to put up with this, stressed Maria.
I thought my pelvic floor issues weren’t that bad, and that other women had it far worse. I’ve interviewed women left with devastating bowel injuries after giving birth, so it seemed acceptable almost to just keep calm and carry on. But during my appointment, which took just over an hour, we addressed a handful of issues, spanning from sex to posture and continence.
Advertisement
Yasmine Ghadache, an osteopath, was also on hand to help. In a weird turn of events, the night before my appointment I somehow managed to pull a muscle in my back and was in a lot of pain – she explained it was likely as a result of me carrying my baby (now a two-stone toddler) repeatedly on one side.
She manipulated the area and within a couple of days, I was back to normal.
Both Yasmine and Maria were very knowledgeable and so passionate. Sitting with them, talking about women’s health, I dared to imagine a world where women got proper postnatal care.
The sessions are up-close-and-personal at points. To check how well my pelvic floor muscles were working, Maria popped a gloved finger into my vagina (she did ask first) and told me to squeeze – all while we had a friendly chat.
Advertisement
During the exam, she discovered I have a very tight internal pelvic floor muscle, which needs some follow-up work. (I’m going to be honest, I didn’t fully know what a pelvic floor muscle was before this session and now we are WELL acquainted.)
Both Maria and Yasmine made me feel incredibly comfortable throughout the process, though. It wasn’t painful at any point. I felt genuinely supported and cared for. These women clearly wanted to help me feel my best.
Roughly one in three women experience urinary incontinence three months after pregnancy, around one in seven experience anal incontinence six months after birth, and one in 12 women report symptoms of pelvic organ prolapse.
All of these issues can affect a woman’s ability to work, as well as their sexual and social relationships, and their mental health.
Mums put everyone but themselves first, but we should also be able to stand up and say: I deserve to feel good about myself, too. If Mummy MOTs were available to every birthing parent on the NHS, well, I think we’d be unstoppable.
Advertisement
Alas, they’re not. But if you have had a baby – whether six weeks or six years ago – and you’ve been struggling with pelvic floor issues, or problems with separated stomach muscles or posture, I would recommend a consultation.
You deserve to have your body back – you’ve certainly given enough.
Graphic content warning: this article includes photos of an injured finger.
The mum of a baby whose fingertip was cut off after it became caught in a folding step stool is urging other parents to be aware of the dangers – and to keep theirs well out of reach of little hands.
Kay de Bruyn, 35, from Alberta in Canada, said she kept a step stool next to the sofa so her eldest son could get on and off it to watch TV.
Advertisement
But one morning, disaster struck when she turned her back for a moment and heard a “thud”, followed by her youngest son, who is one, screaming and crying.
“I had never heard a cry like that before,” de Bruyn told HuffPost UK. “He was lying on his stomach and the stool was now collapsed and lying on the ground in front of him.
“I thought he might have tripped and hit his face on it. But when I picked him up, there was blood everywhere. I caught a glimpse of his middle finger – it looked like the tip was gone.”
Advertisement
Kay de Bruyn
Her son’s finger after the accident (left) and since healing fully (right).
The mum said her son was inconsolable and she began to panic.
“I grabbed a clean cloth from the bathroom and held it to his finger. I wish I could say I stayed calm, but I completely lost it,” she said.
After calling her husband and her parents, she ran across the street with her son and knocked on her neighbour’s door.
Advertisement
“I explained what had happened and asked them to check if the fingertip was truly gone,” she said.
“They gently took my son, checked, and confirmed it. Still holding him, they came back to the house with me and even offered to drive us to the emergency room.”
The parent quickly ran upstairs to see if she could locate the fingertip. “And that’s when I saw it: the tip of his finger was still stuck in the stool,” she recalled.
“I brought the stool downstairs, and my neighbour pried it out using a clean kitchen knife. While he did that, I called emergency services, and they instructed me to place the fingertip in a clean plastic bag.
Advertisement
“The ambulance arrived and took us to the children’s hospital, where they reattached the fingertip. Unfortunately, part of it didn’t survive and eventually fell off.”
Because part of the fingertip is missing, her son’s nail is now growing over the tip of his finger and the family is hoping to get a referral to a plastic surgeon.
“While he seems relatively unfazed by it now, I wanted to share our story – because I know this type of stool is common in many households,” said de Bruyn.
Advertisement
After posting a reel about what happened, the parent said two other families contacted her to say the same thing happened to their children.
“If I had known something like this could happen, I never would have kept it in our home,” she added.
The data is in! The Social Security Administration has released its official list of the most popular baby names of 2024.
For the sixth straight year, the No. 1 name for girls is Olivia, which overtook Emma in 2019. Meanwhile, Liam is still the most popular name for boys for the eight year in a row. Noah and Emma also held steady as the No. 2 names.
The SSA compiles the annual list based on the names parents in the US gave their babies born in the previous year. Although the top name rankings usually don’t super dramatically from year to year, there were a few interesting small changes from 2023 to 2024.
Amelia surpassed Charlotte for the No. 3 spot, Mia jumped up to No. 5 in place of Sophia, and Evelyn knocked Ava down a ranking. Meanwhile, Sofia (with an f) joined the top 10 for the first time ever last year as the 10th most popular name for girls, ousting Luna from the list.
As for the boys, Theodore jumped up three places from No. 7 to No. 4. Henry is now the sixth most popular name for boys, having risen two spots, and Mateo moved down to seventh.
Without further ado, here are the top 10 girls’ and boys’ names of 2024.
In one of his more recent videos, the father-of-three can be seen shushing and bouncing a baby to sleep, before trialling some more, ahem, avant-garde sleep techniques.
“Go to sleep now or I’m going to set fire to this,” says the comedian, while standing next to the cot holding Ewan the sheep.
“I don’t actually want you to go to sleep,” he says in the next breath, trialling a bit of reverse psychology. “I think you should stay up all night.”
Next on the dad’s list of techniques is peer pressure. Perched casually by the side of the cot, stroking his face, he says: “So apparently all the cool babies have been getting early nights recently… Yeah, that’s just what I’ve heard.”
Advertisement
Lewis also trials whale sounds, bargaining and the threat of cancelling Christmas. At one point he’s standing near the cot with a 4-pint bottle of milk.
But it’s the last tip that seems to do the trick: boring his child with chat about Bitcoin.
The 37-year-old from Manchester told HuffPost UK: “My baby isn’t sleeping at the moment so I’ve been desperately searching Instagram and TikTok for advice.
Advertisement
“Once you try everything and it still doesn’t work you start resorting to crazy threats and ultimatums that a baby is obviously not going to understand.
“I thought it’d be funny to do a ‘how to’ video that isn’t particularly helpful but reflects our desperate behaviour as parents.”
Advertisement
Parents dubbed the video “hilarious” and many seemed to think the Bitcoin tip – while a joke – was actually pretty genius.
There were also plenty of suggestions from others about the lengths they’d go to to get their little ones to sleep.
“I used to read books in a really boring voice, then I would fall asleep and they’d stay awake,” said user rachlbc.
“Just put a recording on of the finance review work Teams call,” added hannahlou1983.
Another commenter, nicoledanica, said the video was “spot on”. She added: “I’m a nurse and I used to give detailed lectures to my son about anatomy and physiology when he was a baby and would wake up in the middle of the night.”
My due date was fast approaching when I had a moment of clarity. Or it might have been madness, I’ll let you decide.
I’d been receiving maternity care at a local hospital – the same hospital where my eldest daughter had been born almost three years earlier – and decided I really didn’t want to go back there to give birth.
Advertisement
So, at 34 weeks pregnant, I went online and did what I knew best: researched.
With my laptop perched on my ballooning belly, I looked at other hospitals and saw there were some decent options. But, palms all sweaty, I quickly realised it was the thought of another trip to the labour ward that was filling me with so much dread.
I briefly considered a home birth but realised I wouldn’t be able to relax properly if I knew our neighbours could hear me mooing away (and believe me they would be able to hear it – our walls are paper thin).
Then I saw something intriguing on Instagram of all places: a freestanding NHS birth centre and it was just 10 minutes further than the hospital where I’d been receiving antenatal care. How had I never heard about it?
Advertisement
Why I switched up my care
I’m not a particularly anxious person but the very thought of going back to that first hospital to give birth filled me with dread. Just thinking about it would make my heart race.
The thing is, I had always thought I didn’t have a particularly bad experience at that hospital – compared to the horror stories I’ve heard, it was a “walk in the park”. I was one of the lucky ones. My birth was relatively straightforward: it was a vaginal delivery, no interventions, and my baby was OK.
I experienced some tearing but didn’t really think much of it at the time because it was all quite numb down there. My partner got kicked out a couple of hours after giving birth, which I found to be the most distressing part of all because I had no idea how to look after a baby and was absolutely exhausted.
Advertisement
I remember spending the following 12 hours sat in a bloody hospital gown waiting for my partner to be allowed back into the hospital for visiting hours (cheers, Covid) so I could finally have a shower and hand our newborn over to him.
I was exhausted because I’d barely slept all night – my daughter had been born late the night before, so I’d been up all night checking she was still breathing and listening to the coughs of other mums on the shared ward, hoping they didn’t have Covid. It also happened to be the hottest day of the year which only added to my anxiety.
In the days and weeks after the birth, I experienced some issues with an infection and my stitches coming undone. I also saw a GP at my eight-week follow up appointment who checked my perineal area and suggested my tear had been worse than first thought.
Advertisement
“I was one of the lucky ones. My birth was relatively straightforward: it was a vaginal delivery, no interventions, and my baby was OK.””
I felt I couldn’t really complain about the fact the midwife “popped my vein” – she failed to put a cannula into my arm before I was about to give birth, so we had to wait for a doctor to come and do it. My blood platelets had been on the low side so they thought they’d put a cannula in ahead of time in case I needed a blood transfusion or something – a thought which made me feel really relaxed!
Advertisement
Or the fact that I had to be on a labour ward because of those cursed platelets and all I could hear in the rooms along the corridor were screams.
Or the fact I had two midwives – an experienced staff member and a student – rummaging around in my vagina, one after the other, before delivery. It prompted a panic attack and, I’d argue, was more painful than birth at points. Now, I know midwives are short on time and we all have to learn, but I was not prepared for how painful that examination was going to be. And I wasn’t allowed an epidural because of the platelet issue, so I felt it all.
These things were all unpleasant, but nothing compared to what I’ve heard from other mums. I was a lucky one, right? My baby survived.
I realise now – after years of mentally dismissing what had happened – that perhaps there was a reason why my body was going into fight or flight when I sat down to consider the thought of another hospital birth.
My body was saying no, and thank goodness I listened.
Advertisement
So, at 34 weeks pregnant, I switched up my maternity care. It’s fairly easy to do – I self-referred to the birth centre and then called the hospital and explained I was moving my care across.
I had to do another booking appointment (this is the first appointment you usually do when receiving antenatal care in England, where they check your weight, height, take urine and blood samples, etc.,), but on the whole it was an easy process.
And I cannot stress to you how refreshing it was to speak to the midwives at Edgware Birth Centre.
They were so relaxed and didn’t overly-medicalise things. I asked about my platelets again and they didn’t seem worried – my midwife was so reassuring and, unlike at the hospital where I’d seen a different person each time, this person was someone I spoke to continuously for the following six weeks.
It’s hard to express what a game-changer it was having the same midwife for my antenatal appointments. When we chatted on multiple occasions in the run up to the birth, I felt like I was a human, not just a number who was there to pop out a baby.
Advertisement
On the day I gave birth, I went to the birth centre at around 11am when my contractions were ramping up and called my midwife en route, who amazingly was on shift. They got a room ready for me and started filling the birth pool, as I’d asked if I could try that for pain relief purposes and also to help reduce the risk of tearing again.
When we got there, we went straight to the room and I nearly cried. They’d turned some fairy lights on and there was a diffuser pumping out a calming fragrance in the corner. The birth pool was trickling away. There was nobody screaming in the distance. The atmosphere was so… tranquil.
“Do you want a drink?” my midwife calmly asked me, and then my partner. We looked at each other in disbelief.
Advertisement
Natasha Hinde
The room where I ended up giving birth.
The next few hours were a bit of a blur but consisted of a lot of reassurance from my midwife and her colleague who kept telling me that I knew what I was doing, to listen to my body, and to let them know if I felt an urge to push.
I believe their kindness and reassurance, as well as the feeling of safety from being in this little sanctuary they’d created on my behalf, helped everything speed up a bit and by 2.30pm, our baby was in my arms.
Advertisement
I didn’t need stitches (thank you, birth pool) and by 7pm we were home.
It was a good birth – and I feel bad for saying that, because so many women do not get to have a good birth. I firmly believe that if I hadn’t switched up my care at the eleventh hour, it might not have been a good birth.
And of course, we can never know, but studies have found having a baby at a birth centre is as safe as giving birth in hospital,yet results in fewer interventions.
However, the story doesn’t end there. A few months after I gave birth, I received an email inviting me to join a consultation about the proposed closure of the birth centre. The NHS North Central London Integrated Care System said that, on average, fewer than 50 women give birth there a year.
Advertisement
Under proposed new plans, the birth suites could be closed however the birth centre would still provide antenatal and postnatal services. I couldn’t believe what I was reading.
Deflated by the proposed closure, I attended the online consultation and sat listening to other mothers who had received positive experiences there.
The stories I heard hammered home exactly what can happen if a maternity service isn’t overwhelmed with demand and midwives can truly focus on the people giving birth: they are treated like human beings. The midwives have more to give because they are not physically, mentally and emotionally exhausted.
Advertisement
The decision on the fate of the birth centre is due to be announced this spring.
Dr Jo Sauvage, chief medical officer at North Central London Integrated Care System, told me: “Your positive feedback is a great reflection of the midwifery team at Edgware Birth Centre. We want, above all else, for everyone who gives birth in North Central London to have a similarly high quality of experience, and this means making some difficult decisions.
“The proposed option that we put forward for consultation would see us retain and expand the antenatal and postnatal services at Edgware Birth Centre. For those who choose a midwifery-led birth, we are proposing to maintain the option of home birth, and co-located midwifery-led units which provide a home from home environment.”
Action group Delivering Better is currently calling on the Secretary of State for Health and Social Care, Wes Streeting – who has openly said the maternity crisis keeps him awake at night – to improve maternity care with two key changes: the chance to see the same midwife throughout pregnancy and proactive health checks after the baby is born at three and six months.You can add your voice to the open letter here.
There’s a lot of work to be done when it comes to overhauling the UK’s maternity and postnatal care system – and one birth centre cannot change that. But if it helps women have a good birth, a safe birth, then I’d argue it’s worth its weight in gold.
Advertisement
Update: We have amended the article to clarify that, on average, fewer than 50 women give birth at Edgware Birth Centre each year.
A baby names expert has revealed the ‘vintage’ names she believes will see a resurgence in 2023 and beyond.
Mia Bardot, the editor-in-chief of Random Names, suggested monikers such as Julia, Betty and Vincent could see a revival in the popularity charts as parents look for “timeless classics which evoke nostalgia”.
Advertisement
Celebrities are also exploring the vintage name trend with their new arrivals, which could prompt others to follow suit.
Blake Lively and Ryan Reynolds, for example, have named three of their children James, Betty and Inez. They recently welcomed their fourth child, however it’s not clear what they have named them.
Bardot said: “It is so exciting to see these timeless classics resurfacing. Eleanor, Margaret, Julia, and Adelaide have royal and elegant rings, while Betty and Inez were immensely popular in the 20th century and present a charming simplicity.
“The sturdy and enduring appeal of names such as Henry, James, and Louis is hard to resist due mainly to their deeply rooted royal associations.“
Advertisement
According to experts at Nameberry, the best vintage names are inspired by literary, biblical and royal sources.
Bardot predicts the following names will continue to rise in popularity throughout 2023, thanks to their “elegant and historical feel”.
A video of a baby interacting with their dad is melting hearts across the internet – and while it’s certainly got the cuteness factor, there’s also a very important lesson behind the video which an early years expert has shared.
The expert suggested this interaction helps “light up” a baby’s brain. He calls it “serve and return” – yes, like in a tennis match.
“Serve and return entails back and forth interaction during which adult and child trade conversational (and other expressive) turns,” Wuori explained.
The video shows the baby sticking her tongue out – which the early years expert described as a “serve”. The dad then “returns” by copying the expression, but also “extending her cues and vocalisations”.
According to Harvard University’s Center on the Developing Child, these ‘serve and return’ interactions shape brain architecture, help build relationships, and their absence “is a serious threat to a child’s development and well-being”.
This is why Wuori’s message was ultimately for parents to do as much interacting, face-to-face, with their baby and child as possible, which means being mindful of screen time and other distractions.
And no, this doesn’t mean watching them like a hawk 24/7, but rather taking time out to really connect with them, with zero distractions, throughout the day.
With babies, some examples of “serve and return” interactions might include:
If your baby smiles and you smile back at them
If they make a sound and you mimic the sound
If they look at something and you explain what it is.
If your child points at something, or seems interested in something, pay attention to what they’re focused on. This will help you learn more about your child’s abilities, interests and needs.
Offer children comfort with a hug and gentle words, help them, play with them, or acknowledge them. So, for instance, you could make a sound or facial expression, or nod, to let a child know you’re noticing the same thing.
Help name what your child is seeing, doing or feeling to help them learn to talk and understand words.
Take turns with them while playing or drawing, as this helps them learn self-control and how to play with others.
So, next time you’re in the presence of a baby or young child, you know what to do.
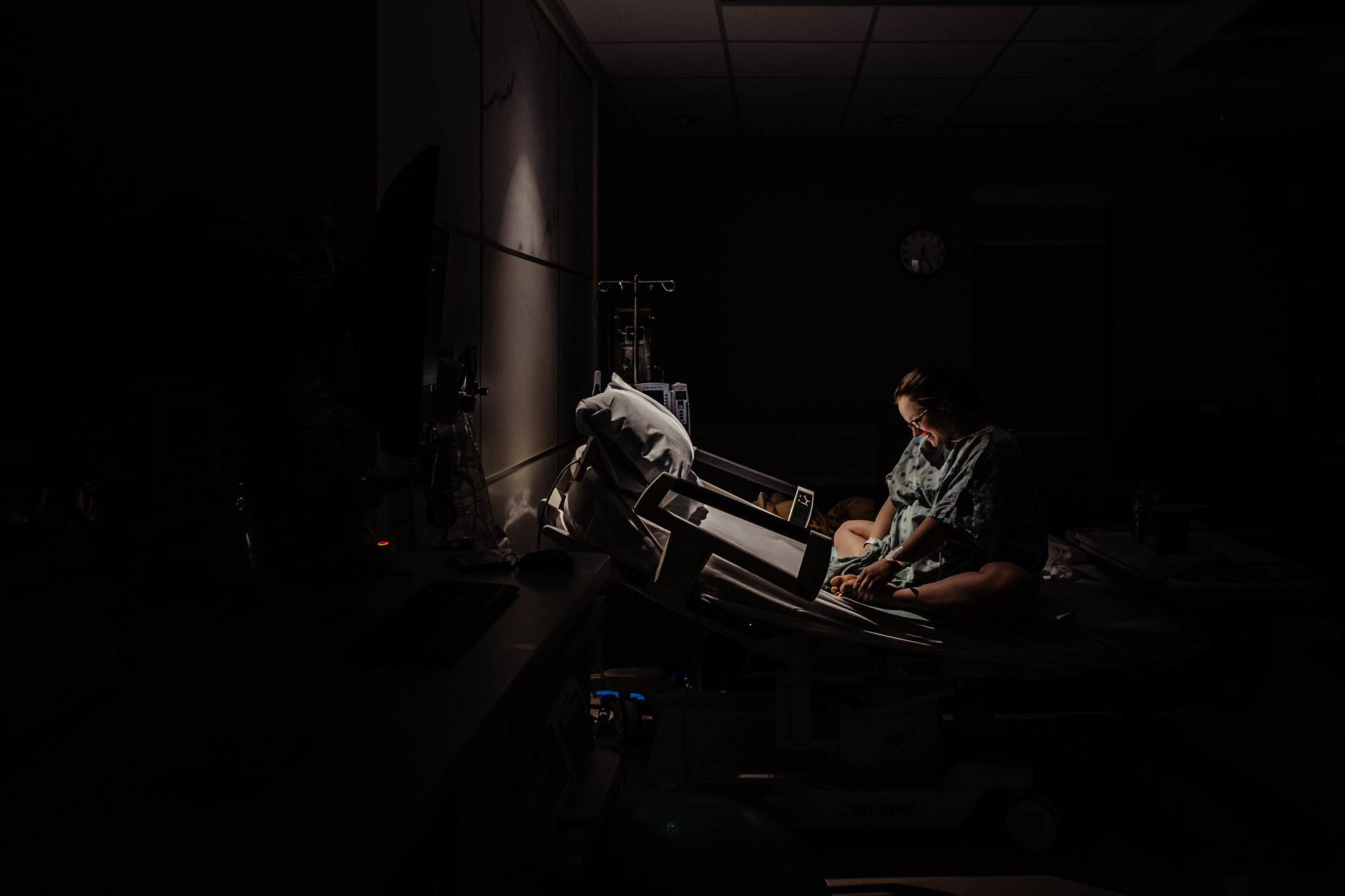
The photographers who document childbirth capture some of the most powerful and emotional moments in a parent’s life.
The organisation invited birth photographers to submit photos taken in 2022 and 2023 and received entries from almost 200 photographers around the world.
A panel of judges selected winners in categories like “between two worlds,” “birth team,” and “story in one image.”
“We put together this year’s showcase because we wanted to find a way to celebrate powerful birth imagery in a new way,” Nicole told HuffPost.
“By creating some more unique categories, we hoped to shine a light on images that often get overlooked in traditional photo contests.”
In addition to fostering a sense of community among birth photographers, Mason and Nicole work to change policies on social media platforms and offer courses for aspiring birth photographers.
Their biggest goal, however, is to make birth more visible, which they believe will help create a “safer and gentler” experience for all.
“We hope that people feel inspired by the images they see, and we hope they can recognise themselves or their birth story in some of these images,” Nicole said.
“We hope that this entire showcase illustrates just how diverse, powerful, and beautiful birth can be. ”
Keep scrolling for a selection of winning photos and other submissions and visit Birth Becomes You for the full collection. (Readers should note that the following uncensored photos show people in the act of childbirth.)