As I write this I can feel another illness taking hold: the headache, the stuffy nose, the scratchy throat. It can only mean one thing: the kids are back at school!
While plenty of people will be relieved to get back to normality after two weeks of juggling work and childcare, a survey of 1,000 parents by Olbas found over half (55%) dread their kids going back to school due to the increased chance of getting ill.
Advertisement
There’s no getting around it, they will (probably) get sick in the coming fortnight.
Dr Roger Henderson, an NHS GP and spokesperson for Olbas, says: “When children return to school after Easter holidays or extended breaks, it’s normal to see a sudden rise in sniffles, coughs, and stomach upsets.
“This isn’t because schools are unhealthy places, but rather because children are suddenly exposed to lots of germs they haven’t encountered in a while – almost like a refresher course for their immune systems!”
“Parents should expect a wave of minor illnesses and be prepared with tissues, comfort foods, and perhaps a flexible routine to allow for extra rest,” says the doctor.
“The good news is that these minor illnesses help children build up stronger immune systems over time. While it can feel overwhelming at first, most of the common viral illnesses pass quickly, and children normally bounce back with their usual energy.”
Advertisement
Here, Dr Henderson shares some tips and tricks to overhaul your morning routine to at least give everyone a fighting chance amid the post-holiday bug surge.
1. Create a 10-15 minute buffer zone
The GP is a firm believer in creating a 10-15 minute ‘buffer zone’ on those mornings when the kids are waking up sniffly.
“Building in a ‘buffer zone’ of 10-15 extra minutes can ease stress and reduce the chance of forgotten items or unexpected delays affecting you.”
2. Start the day with a warm shower or saline spray
If your kids are particularly congested first thing, a warm shower or saline nasal spray can help clear clogged sinuses and “make them feel fresher” for the day ahead.
3. Keep breakfast simple
When kids are feeling below par, something simple and nourishing to set them up for the day can work wonders. Dr Henderson suggests porridge, scrambled eggs, or smoothies are “easy options that don’t require much fuss”.
Advertisement
4. Take a calmer approach to rushed mornings
Easier said than done when you’ve got to be at work for 9am, but if kids aren’t feeling great, they’re going to require a bit more patience in the mornings. The GP says a “calm reassuring tone sets the pace here”.
When to keep your child off school
While kids can go to school with coughs and colds, there are instances where you shouldn’t send your child to school. Here’s what NHS Choices advises:
If they have a fever, keep them off until the fever goes away.
If they have a high temperature, keep them off school until it goes away.
If they have diarrhoea or vomiting they should stay away from school until they have not been sick or had diarrhoea for at least 48 hours.
If they have chickenpox, keep them off school until all the spots have crusted over – usually about five days after the spots first appeared.
If they have symptoms of Covid-19 including a high temperature, and they don’t feel well enough to go to school or do normal activities, keep them off.
If your child has an ear infection and a high temperature or severe earache, keep them off school until they’re feeling better or the high temperature goes away.
If your child has impetigo, they’ll need treatment from a GP – usually antibiotics. Keep them off school until all the sores have crusted over and healed, or for 48 hours after they start antibiotic treatment.
If your child has scarlet fever, they’ll need treatment with antibiotics from a GP. Otherwise they’ll be infectious for two to three weeks. Children can go back to school 24 hours after starting antibiotics, providing they feel well enough.
This article features advice from Dr Tom Nutt, of Meningitis Now, Professor Adam Finn of the University of Bristol, and Professor Emma Wall, clinical professor of infectious diseases at Queen Mary University of London.
The meningitis outbreak among students in Kent has included cases of B meningococcal disease, sometimes known as MenB,
Advertisement
On Tuesday, the UK Health Security Agency (UKHSA) said it was continuing to investigate the outbreak – with four laboratory cases confirmed and 11 under investigation. This includes two people who have died.
Group B meningococcal disease can cause serious illness, including severe inflammation of the brain membrane (meningitis) and blood poisoning (septicaemia), which can prove fatal.
Most teens and adults aren’t vaccinated against MenB
Meningitis most commonly occurs in babies, young children, teens and young adults.
There are three vaccines which protect against the main causes of meningitis.
The MenB vaccine is offered to infants at eight weeks, 16 weeks and one year of age, as part of routine NHS vaccinations – this came into play in 2015 so anyone under 10 has some protection.
Advertisement
Babies are also given the pneumococcal vaccine at 16 weeks and one year.
The MenACWY vaccine protects teenagers against four types of bacteria linked to meningitis and is usually given in school during Year 9 (when kids are aged 13-14).
But the latter vaccine doesn’t protect teens from MenB, experts have warned.
Most teenagers and adults aren’t protected against it unless they’ve paid privately for a vaccine on the high street.
Charity calls for MenB to be added to routine vaccinations for teens
Meningitis Now’s chief executive Dr Tom Nutt noted there are “gaps” in the NHS immunisation schedule, particularly around MenB.
Advertisement
“We are campaigning for the MenB vaccination to be made more widely available to those at risk, especially teenagers and young adults,” he told HuffPost UK.
He noted that vaccines “are the only way to prevent meningitis” – that said, he caveated that “vaccines do not protect against all causes of meningitis and no vaccine is 100% effective”.
Prof Adam Finn, Professor Emeritus of Paediatrics at University of Bristol, added that protection from the vaccine “lasts for some years, but not forever”.
Advertisement
The MenB vaccines also do not “reduce carriage and transmissions of the bacterium,” he noted, meaning you could have the vaccine and still carry or transmit the bacteria to others.
Ultimately, it’s important that people make themselves aware of the signs and symptoms of meningitis, and to get immediate medical help if they suspect themselves or a loved one could have it.
Early symptoms, which may not always be present, include:
a rash that does not fade when pressed with a glass
sudden onset of high fever
severe and worsening headache
stiff neck
vomiting and diarrhoea
joint and muscle pain
dislike of bright lights
very cold hands and feet
seizures
confusion/delirium
extreme sleepiness/difficulty waking
Anyone with these symptoms is urged to seek medical help immediately by contacting a GP, calling NHS 111 or dialling 999 in an emergency.
“Despite what has happened in Kent, we would like to reiterate that meningitis is a relatively rare disease,” said Dr Nutt.
Advertisement
“In the long-run, the good news is that the NHS vaccination programme has been very successful in bringing down the number of cases of meningitis in the UK.”
These include: a MenB vaccination given to all those at most risk of disease; a MenB booster programme to protect adolescents by 2030; and availability of the MenB vaccination on the high street at a fair price.
Advertisement
What happens now?
Health officials are continuing to monitor the situation in Kent.
UKHSA confirmed a small targeted vaccination programme will begin among students resident at Canterbury Campus Halls of Residence at the University of Kent.
Professor Emma Wall, clinical professor of infectious diseases at Queen Mary University of London, explained that UKHSA might do this to “reduce the risk of a further outbreak, or shut down transmission (so-called ring vaccination)”.
The vaccination programme may be expanded further as UKHSA continues to asses ongoing risk.
As some of the cases visited Club Chemistry in Canterbury between 5-7 March prior to becoming unwell, UKHSA is urging anyone who visited the club during this time to come forward for preventative antibiotic treatment as a precautionary measure.
Advertisement
HuffPost UK has contacted the Department of Health and Social Care (DHSC) about whether there are plans to add Men B to the routine teen vaccine.
On 1 December 2021, Benedict Blythe went to school, as normal, yet a few hours later, his dad Peter received a call to say he’d been sick. When he arrived to pick up his son, it became clear he was seriously unwell.
Advertisement
Peter began CPR until an ambulance arrived. Sadly, despite medical help, Benedict was pronounced dead in hospital just after lunchtime.
An inquest into his death determined the five-year-old died from an accidental exposure to cow’s milk protein, which triggered fatal anaphylaxis.
His parents, Helen and Peter, have been fiercely campaigning for safety changes in schools ever since.
Advertisement
The couple have worked with clinicians, coroners, charities and parliamentarians to highlight gaps in allergy safety in schools and push for national protections so no other family suffers a similar fate.
And now it seems ‘Benedict’s Law’ is set to make real change.
The government has shared that under new statutory guidance, schools will have to stock life-saving adrenaline auto-injector pens, teachers will undergo compulsory allergy awareness training, and every school will need to have a dedicated allergy policy.
The guidance is currently open for consultation and will come into force in September 2026.
Helen and Peter said: “We are grateful that the government has listened to us, and that as a result a new generation of children with allergies will, from September, enter a school system far safer for them.
Advertisement
“Our son Benedict died aged just five years old, from an allergic reaction in school that was not only preventable but treatable.”
They added that if Benedict’s Law had been in place when their son joined his school, “he may still be alive”.
Helen and Peter Blythe, pictured with their children.
Advertisement
Food allergy affects around 7-8% of children worldwide, equivalent to roughly two pupils in every classroom. What’s more, roughly 30% of allergic reactions in schools occur in children previously undiagnosed with an allergy.
“As a family, leading the campaign for allergy safety in schools has been about remembering our son,” Helen and Peter continued.
Advertisement
“He was a kind, clever boy who cared about helping others – so knowing that for the first time schools will be expected to protect children with allergies like him from harm feels like a fitting legacy for Benedict.”
The Benedict Blythe Foundation caveated that while guidance sets expectations, it does not create an enforceable legal duty or guarantee consistent implementation across every school.
Olivia Bailey, minister for Early Education, said: “No parent should have to send their child to school worried that a life-threatening allergic reaction won’t be handled swiftly.
Advertisement
“We have listened to the families and organisations who have campaigned tirelessly on this issue, and we are acting.
“These new requirements will give parents the confidence that every school has the training, the plans and the equipment in place to keep their child safe.”
Tanya Ednan-Laperouse OBE, whose daughter Natasha died aged 15 from an allergic reaction, said she is “deeply grateful” that the government is taking action to keep children with food allergies safe at school.
Measles cases continue to rise in London, largely driven by an outbreak of the illness among children in Enfield.
There have been 50 confirmed cases of measles in the borough up to 16 February, according to the UK Health Security Agency (UKHSA). However, experts have said it’s likely the actual number of cases will be higher.
Advertisement
The outbreak is mostly affecting unvaccinated children under the age of 10, in both schools and nurseries.
According to a GP surgery in Enfield, one in five children with measles have been hospitalised as a result of this latest outbreak, and all of those hospitalised have not been fully immunised.
For a number of years, the borough has struggled with low uptake of the measles, mumps and rubella (MMR) vaccine – which children can have two doses of in early childhood as part of NHS immunisations – due to online misinformation, health equalities and general vaccine hesitancy, the Guardian reported.
Advertisement
On 19 Feb, Dr Vanessa Saliba, consultant epidemiologist at UKHSA, confirmed the outbreak has led to some children ending up in hospital.
The possible long-term health complications from catching measles can include: hearing loss, blindness, pneumonia (infected inflammation of the lungs), encephalitis (inflammation and swelling of the brain) and brain damage. In some cases, it can prove fatal.
“Measles is a nasty illness for any child, but for some it can lead to serious long term complications and tragically death, but is so easily preventable with two doses of the MMRV vaccine [the MMR vaccine also now includes protection against varicella, or chickenpox],” Dr Saliba said.
Advertisement
“All parents want what is best for their child – if they have missed any of their doses or you’re unsure, get in touch with your GP surgery. It’s never too late to catch up.
“The MMRV vaccine will give them the vital protection they need against this highly contagious disease, and also help protect more vulnerable children around them who are too young or unable to have the vaccine due a weakened immune system.”
Symptoms of measles
Measles typically starts off like a cold with a high temperature, runny nose, sneezing, cough and red, sore, watery eyes.
Advertisement
Some people might also experience Koplik spots, which show up as white spots inside the mouth on the inner lining of the cheek and lips – this can help distinguish it from a common cold.
The distinctive body rash can show up a number of days later. This is the “most typical symptom of measles, which usually starts on the face and spreads to the rest of the body”, Superdrug’s pharmacy superintendent Niamh McMillan previously told HuffPost UK.
“It usually appears three to five days after first signs of symptoms and lasts for several days. The rash can be flat or slightly raised and join together into larger patches.”
Advertisement
According to the NHS, the rash can look brown or red on white skin and may be harder to see on brown and black skin.
If you suspect your child has measles, the NHS advises to call for an urgent GP appointment or to speak to NHS 111. It’s important to call your GP surgery before you go in as measles is very contagious.
In My Story, readers share their unique, life-changing experiences. This week we hear from Richard Poulin, 40, who currently lives in Bangkok, Thailand.
My wife and I accepted new teaching jobs in Singapore. Before leaving America, we proudly showed our newborn daughter, Rylae-Ann, to family. All was right in the world, and we eagerly boarded a plane to begin our new life.
Advertisement
However, when Rylae-Ann was three months old, we saw signs that all was not right.
She was missing developmental milestones. We would play games to encourage her to reach out, do exercises to practice sitting independently, and give massages to coax her to engage her core muscles. But nothing seemed to work.
One day my wife, Judy, went to look for homes while I stayed back at the hotel with our daughter. During one of the sessions, Rylae-Ann tensed her arms and legs. Her eyes briefly crossed, and her tongue made a thrusting action.
Despite it lasting a few seconds, I was concerned. I attributed it to my pushing her too hard, causing muscle cramps. I tapered my eagerness for my daughter to progress.
The fleeting actions caused enough concern that I did some Googling. I did not dare tell Judy. I didn’t want her to start worrying.
Advertisement
I came across an article about a girl with a deadly ultra-rare disease. I admonished myself. I had become one of those parents who Googled symptoms and ended up with an obscure diagnosis for my daughter. I closed my laptop and tried to focus on my family’s new life in Singapore.
Richard Poulin
As the days passed, Rylae-Ann’s parents realised she was missing developmental milestones.
Over the next few months, our lives began to unravel. The tensing of muscles in our daughter’s tiny limbs became more intense and lasted longer; it was the only time we ever saw any movement from her.
We began to refer to them as ‘spells’. These spells came every three days like clockwork. She had trouble staying asleep. When she was awake, she looked sleepy and constantly cried.
Rylae-Ann’s developmental milestones remained paused at the three-month mark. She couldn’t hold up her head, she did not reach out and grasp things, and her eyes remained tiny slits. The photographer commented on her sleepy look when we got her identification card.
Advertisement
We went to doctors who reassured us that babies develop at different rates. But as the spells’ intensity and duration grew, we could no longer sit idly by. We began visiting more doctors and researching.
One rainy night, the spell lasted longer and was more intense – we were filled with fear. We rushed out of the door to the car we’d booked on a ride-sharing app and headed to the nearest hospital. I willed all the lights to turn green while Judy cooed softly into Rylae-Ann’s ear. Once we arrived, the nurses did an assessment and put our daughter at the front of the triage line.
They gave our daughter diazepam for fear she would have another seizure. A doctor came and assigned an initial assessment of epilepsy. The doctors admitted Rylae-Ann, and we were separated from her for the first time.
Judy and I discussed the diagnosis when we returned home to get clothes and necessities. What the doctor was telling us didn’t seem right, mainly because we thought what the doctor saw as a seizure was something else due to its three-day cyclical nature.
Advertisement
After a barrage of tests, the doctors said she had epilepsy. They prescribed her medication, and we went home. But her symptoms did not improve. The medicine left her sleeping all day and she felt lifeless when we picked her up – we stopped the drug after a few days.
We continued to visit the doctor, trying to explain why we thought it wasn’t epilepsy. Despite genetic testing, blood tests, EEGs (which record brain activity), MRI, CSF (cerebrospinal fluid) tests, and more coming back normal or inconclusive, the doctors did not change their diagnosis, so we went to other doctors. We even travelled to other countries searching for answers.
As we collected second opinions, we improved our description and came armed with digital evidence. Doctors had different opinions, including epilepsy, dystonia, cerebral palsy, and other neurotransmitter disorders. However, no definitive answer came.
Our daughter was regularly admitted to emergency care during the onslaught of medical tests. We were always in the hospital, so much so, the nurses knew our daughter by name. Most were lung-related issues such as aspiration, pneumonia, and collapsed lung. But also, a typical childhood viral infection would cause her to be extremely weak to the point that the doctors required her to be in intensive care.
Answers never came. Instead, a random Facebook post about a child with similar symptoms caught the eye of Judy’s older brother. When Judy shared the article with me, it triggered a memory of a post I saw earlier.
The name AADC stuck with me because of its similarity to a classic rock band. I remember the article discussing the extremely rare disease, affecting around 130 people worldwide since 1990.
Advertisement
Richard Poulin
Rylae-Ann would often end up in intensive care.
I explained how it was improbable. However, Judy pointed out that although it is an extremely rare genetic disorder, many of the children were from Taiwan, where her parents are from.
AADC deficiency is a rare disease that causes a mutation in the DDC gene. This gene instructs the body to produce the AADC enzyme, which is responsible for dopamine and serotonin.
Children with AADC deficiency have little or no dopamine and serotonin. Both are responsible for several critical bodily functions to sustain life and movement.
That night, alarms were going off in my head. I sat up in bed and went to work, reading research papers about the disease. The more I read, the more I knew our daughter had this. One glaring reality was that children with this disease die early in life due to the severity of the symptoms.
Advertisement
One of the reports talked about how a doctor in Taiwan had completed clinical trials for an experimental, innovative treatment. There was no word if the treatment was available, but I knew we had to visit this doctor.
Richard Poulin
Rylae-Ann struggled to sit upright or feed.
Judy’s younger brother still lived in Taiwan, so we asked him to make an appointment as soon as possible. The next day he told us we had an appointment booked a week later, the day after Christmas.
We packed our bags and landed in Taiwan on Christmas day. That night, Judy and I sat at the park drinking a small bottle of vodka, trying to process how we went from cloud nine, to falling from a cliff, to Hell over six months. As the bottle’s contents disappeared, I promised my wife we would never have a Christmas like this again.
On the day of our appointment, we met the doctor who was surprised to receive patients thinking their child had a rare disease – and even more surprised at our knowledge of the disease.
“The doctor felt confident that our daughter did, in fact, have an aromatic L-amino decarboxylase (AADC) deficiency.”
I asked if the treatment in the article was available. We held our breath. “No,” he replied. Tears welled. “But, there is another clinical trial recruiting. However, it is only available for Taiwanese.”
“She is Taiwanese!” we screamed. We had recently applied for her citizenship. Although Judy is Taiwanese, she never lived there. We grew up in Thailand, where Rylae-Ann was born. Rylae-Ann only had an American passport, but her Taiwanese passport would soon be ready.
She enrolled in the clinical trial for a new exploratory treatment known as gene therapy. However, she had to wait 11 months to begin treatment – another year of trying to keep her alive and healthy.
Advertisement
Yet with the mystery uncovered, we had more information on how to care for her.
The 11 months also gave us time to figure out the logistics of how our daughter would participate in the study. She would have to stay in Taiwan for six months, so we decided to have Judy’s mum and nanny remain in Taiwan for that period while Judy and I took turns flying back so we could continue earning money at our new jobs in Singapore.
Richard Poulin
Judy and Rylae-Ann on the day of her surgery.
On 13 November, when Rylae-Ann was 18 months old, she underwent brain surgery for gene therapy. Family and friends asked us if we were worried. We weren’t. We had our backs against the wall and fought to keep our daughter alive.
While alive, she depended on us for everything. Managing work to pay the mounting health care bills was extremely difficult. There was no downtime or social life. I remember telling Judy that the lack of sleep was making me mad.
We felt blessed that our daughter would have an opportunity in life.
The surgery lasted several hours. It was Judy’s turn to be in Taiwan, so I waited for a video chat update.
Advertisement
The way we explain gene therapy to other parents is it involves injecting a shell of a virus into the brain. The virus normally goes unnoticed by the body, so it is able to bypass the body’s immune system. Researchers used this situation to inject good DNA into the virus. The virus then “infects” the good DNA in the body. In our daughter’s case, it was in the area of the brain where dopamine is produced.
The surgery was a success. A few days later, to Judy’s surprise, Rylae-Ann was discharged. We began physical therapy immediately.
The results came quickly. One month later, she sat up on her own. This was a huge milestone. Since then, she has continued to make progress. Every day we supported her, but we did it in a way where we could still make memories as a family.
Just over a year after gene therapy, our daughter was swimming, walking, running, and even riding a horse. Today, she is an independent child who continues to explore the world. Not only does our daughter have a chance to live, but we also have a chance to be parents.
Richard Poulin
Rylae-Ann has grown into an independent child who continues to explore the world.
Advertisement
Judy and Rich now use their spare time to help other families in the rare disease community and have launched a non-profit organisation called Teach RARE, where they work to raise awareness and teach caregivers how to combine educational activities with therapy goals.
To take part in HuffPost UK’s My Story series, email uklife@huffpost.com.
Tens of thousands of children are set to receive hospital-level care at home as part of an expansion of virtual wards on the NHS.
The announcement is set to come from NHS chief executive Amanda Pritchard on the 75 anniversary of the health service.
Advertisement
The ‘hospital at home’ service will cover children in every region of England from this month, after successfully treating more than 6,400 children in a pilot scheme over the last year.
Pritchard said the NHS virtual wards programme has “provided peace of mind” to parents who have used them during trials, including in Blackpool, Dudley and Dorset.
What is a virtual ward and how does it work?
Virtual wards allow patients to get hospital-level care at home safely and in familiar surroundings, helping speed up their recovery while freeing up hospital beds.
Children on a virtual ward would be cared for by a multi-skilled team who can provide a range of tests and treatments, including blood tests, prescribing medication or administering fluids through an intravenous drip.
Advertisement
They would be reviewed daily by the clinical team and the ‘ward round’ may involve a home visit or take place through video calls.
Many virtual wards use technology like apps, wearables and other medical devices enabling clinical staff to easily check in and monitor patients’ recovery.
Children will be treated for a range of conditions like respiratory illness, such as asthma, and heart conditions, but from the comfort of their homes.
How is it helping children?
In Blackpool, almost 200 children have been treated on a paediatric virtual ward.
Hope Ezard, who is 21 months old, is one of them. She was born prematurely at just 29-weeks and has a rare neurodevelopmental disorder, GNB5, as well as chronic lung disease and feeding issues.
Hope has been in and out of hospital for most of her life to be treated for recurring respiratory infections, and to receive high-pressure oxygen and antibiotics.
Advertisement
The introduction of the virtual ward meant Hope could be moved home sooner.
Hope’s mum, Sarah, 39, said being able to receive care at home “is so beneficial to Hope, and our other children”.
“We know that in general, Hope doesn’t sleep very well when she’s in hospital and is more vulnerable to hospital infections, so there is peace of mind when she’s being cared for at home, on the virtual ward,” she said.
“She’s less likely to pick up anything that might make her more poorly, and she’s relaxed and comfortable in her own bed.
“And the fact that the brilliant community nurses are just a phone call away reduces any anxieties that we might have had.”
In Dudley, mum Anum Shazady praised the virtual ward for keeping her son out of hospital, with twice daily calls from NHS staff.
Advertisement
Anum said: “Now my son is on the virtual ward I can record his observations as many times as I want throughout the day, recording them onto the virtual ward pad and a member of staff calls me twice daily which reassures me that he is safe in our home environment.
“The new virtual ward is great for me and my family as it stops my son staying in hospital longer than he needs.”
Why are they expanding the scheme?
The ultimate aim is to free up hospital beds – especially ahead of winter.
NHS chief executive Amanda Pritchard said: “Virtual wards are already providing excellent care to families when their children are sick, and this expansion will enable thousands more to receive high quality care from home.
“Being treated at home can have a hugely positive impact on patients – it means they receive hospital-level care, but it also means they are not separated from their families – providing peace of mind for loved ones.
“As we look to the next 75 years of the NHS, we will continue to embrace the latest technologies and innovations to meet the changing needs of patients while ensuring that care is as convenient as possible.”
Swabbing newborn babies with their mum’s vaginal bacteria might boost their early development, according to new research.
Known as vaginal seeding, the process involves transferring vaginal bacteria to a baby after a caesarean section, with a view to improving their gut bacteria.
Advertisement
The process reportedly originated in Australia, however over the years has become increasingly popular in the UK, too – with more and more mums asking for vaginal seeding after a C-section birth.
But there are risks attached – specifically the risk of passing on an infection from mother to child.
What is vaginal seeding all about then?
Previous research has found babies born by C-section tend to have different gut bacteria to those born vaginally.
Vaginally born babies receive their early gut bacteria from the mother’s birth canal, while C-section babies’ microbiota are dominated by bacteria found on the mums’ skin, in breastmilk and in the environment.
Advertisement
While the difference tends to disappear as they age, researchers suggest early gut microbiota is associated with the development of baby’s immune system and could affect their disease risk later in life.
This has led to practices like vaginal seeding – basically, mums (or dads) would rub newborns with a gauze swab containing their mother’s vaginal fluids after birth via C-section.
But there is limited clinical evidence that vaginal seeding is safe and effective.
What are the risks of vaginal seeding?
Doctors have previously warned that the process could put babies at risk of infection – particularly from group B strep (GBS), which can prove deadly in some cases. And according to Jane Plumb, chief executive of Group B Strep Support, testing for group B strep “is rarely available in the NHS”.
“[GBS] is carried by around one in four pregnant women, and although it poses no risk to the mother it can cause fatal infections in babies,” Dr Aubrey Cunnington, a clinical senior lecturer from Imperial College London, wrote in the BMJ.
“There are also other conditions that cause no symptoms in the mother, such as chlamydia, gonorrhoea and herpes simplex virus, that could be transferred on the swab.”
Advertisement
He spoke about how one colleague had to intervene when a mother with genital herpes, who had undergone a C-section and was about to undertake the process.
“Swabbing would have potentially transferred the herpes virus to the baby,” said Dr Cunnington.
What does the new study say?
Researchers rubbed the lips, skin and hands of 32 newborns delivered via C-section with a gauze soaked with their mothers’ vaginal fluids and another 36 newborns with a gauze soaked with saline as blind controls.
Because of the risks attached, the mothers were tested in advance to make sure they were free of infections, such as sexually transmitted diseases and group B strep.
The team found that newborns who received the microbiota had more gut bacteria found in maternal vaginal fluid six weeks after birth, suggesting that maternal vaginal bacteria successfully reached and colonised babies’ guts.
Compared with C-section newborns who received saline gauze, babies with microbial transfer had more mature bacteria in their guts at six weeks old, similar to babies born vaginally.
Advertisement
And no infants experienced severe adverse events during the experiment, according to the study which was published in the journal Cell Host & Microbe.
It could also boost development
The team also evaluated the babies’ neurodevelopment at three months and six months after birth, using a questionnaire.
They asked the mothers if their babies were able to make simple sounds or perform movements like crawling on their hands and knees.
Babies who had been swapped with vaginal fluid scored significantly higher in neurodevelopment at both ages, and their scores were comparable to those of vaginally born babies.
Study author Yan He, of Southern Medical University in Guangzhou, China, said they now want to determine if vaginal microbiota seeding has the potential to reduce the risk of neurodevelopmental disorders in children, such as ADHD, ASD, and intellectual disabilities.
Advertisement
“It is somewhat like faecal microbiota transplantation,” continued He.
“We need more data to understand this intervention and make it more precise. We may eventually uncover what exactly is beneficial in maternal vaginal microbiota, which could enable us to design therapeutics for all infants born via C-section in the future.”
You’ve likely heard talk in the news about XBB1.5, an Omicron variant that has become a dominant strain of the Covid-19 virus in the US and that experts warn could soon become so in the UK, too.
While for the most part this Omicron variant is similar to previous ones, there are a few things to know about XBB1.5, especially if you believe that it may have hit your household.
What symptoms of XBB1.5 are common in children?
Experts agree that symptoms tend to be the same as those we’ve seen before.
“I have not seen any evidence to suggest the main symptoms of XBB variant are different from previous variants,” Dr. Ruth Kanthula, a paediatric infectious diseases specialist at MedStar Health, tells HuffPost.
“It’s hard to tell about loss of taste and smell in young kids,” says Dr. Tanya Altman, a paediatrician and author of Baby and Toddler Basics.
Advertisement
Altman says she has noticed that kids tend to be less interested in eating while they are sick, and ask for “more flavourful or spicy foods after they recover, which to me suggests their taste may not have fully recovered yet.”
Altman describes the majority of Covid infections that she is seeing now as mild – with kids having less serious symptoms than adults, such as shortness of breath. She adds that children seem to be recovering quickly after testing positive.
“This could be due to the fact that most of the population has some sort of immunity from previous infections or vaccines, or the virus is now weaker, and I think it’s likely a combination of both,” she continues.
It’s important to note, however, that a child can have two respiratory viruses at the same time, which may cause their symptoms to be more severe. Other viruses in heavy circulation right now include RSV and the flu, which some have dubbed, along with Covid-19, the “tripledemic”.
Advertisement
How contagious is XBB1.5?
The “main difference that has been observed with XBB variant compared to other Covid-19 variants is that XBB variant spreads quickly,” says Kanthula.
Advertisement
Because the XBB1.5 variant has quickly come to account for a large portion of infections, scientists think that it may be more highly transmissible than other variants.
Phynart Studio via Getty Images
mother having video call with a pediatrician while holding ill daughter in her lap.
“The XBB.1.5 variant has a mutation virologists believe is helping the virus better bind to cells and thus be more transmissible,” Johns Hopkins professor of molecular microbiology and immunology Andy Pekosz explained in a Q&A on the university’s website.
Practically, this means that the virus could infect many members of a household, or a school classroom, in a short amount of time.
In addition to being more highly transmissible, XBB1.5 also seems to be “immune-evasive,” according to Pekosz, meaning that there may be a lot of breakthrough infections in people who have previously had Covid, are immunised, or both.
Advertisement
What should I do if I think my child has XBB1.5?
If your child has any of the symptoms listed above, it makes sense to give them a Covid-19 test. Note that these tests will only tell you whether your child is positive for Covid-19, not which viral strain they have.
Treat your child’s symptoms just as you would any other respiratory virus, with rest, fluids and acetaminophen/ibuprofen for fever or aches. As always, says Altman, if your child has a fever for more than four days, isn’t keeping fluids down, has trouble breathing or looks really sick, call your doctor.
For infants under three months, you should contact your doctor if they have a fever of 38°C or higher or miss two feeds, as young infants can become very sick with different respiratory viruses.
Does my child need to quarantine if they are infected?
As the NHS website explains, you have Covid-19, you can pass on the virus to other people for up to 10 days from when your infection starts. Many people will no longer be infectious to others after five days.
Anyone with Covid is currently advised by the NHS to try to stay at home and avoid contact with other people for five days, and avoid meeting people at higher risk from Covid-19 for 10 days, even if those people have had a Covid-19 vaccine.
Advertisement
“If a child or young person aged 18 or under tests positive for Covid-19, they should try to stay at home and avoid contact with other people for 3 days. This starts from the day after they did the test,” the guidance continues.
“Children and young people tend to be infectious to others for less time than adults. If they’re well and do not have a temperature after 3 days, there’s a much lower risk that they’ll pass on Covid-19 to others.”
While it’s frustrating to have to keep your child home from school, particularly if they’re not feeling ill, Altman says: “Covid is one that you really don’t want to spread to others, especially those who are high risk, so please keep your kids home when sick, mask if you need to leave your house with sick kids and keep them away from others as much as possible.”
How can I prevent my child from getting XBB1.5?
“I think the goal now is to learn to live with Covid, just as we live with flu, RSV and other contagious respiratory illnesses,” says Altman.
Stay home when sick, wash hands, disinfect surfaces, teach kids to cover their faces when they cough or sneeze, and mask when appropriate (such as days six to 10 of a Covid-19 infection.)
Advertisement
Even though XBB1.5 is known to evade immunity, “based on past experience we know that vaccination can protect against developing severe disease,” says Kanthula, so you should make sure your children have been vaccinated and had boosters.
Altman says she believes that the hybrid immunity of three doses of vaccination and one illness seems to offer the most protection against reinfection.
Experts are still learning about Covid-19. The information in this story is what was known or available at the time of publication, but guidance could change as scientists discover more about the virus.To keep up to date with health advice and cases in your area, visit gov.uk/coronavirus and nhs.uk
Families across the UK have been urged to stay vigilant about Strep A symptoms this week, following a series of tragic deaths in children.
A total of 15 children have now died in the UK from Strep A since September, according to the latest figures. This includes 13 children under the age 15 in England and two others in Northern Ireland and Wales, according to data from the UK Health Security Agency (UKHSA).
Advertisement
Streptococcus A (Strep A – also known as Group A Strep or GAS) are a group of bacteria that can cause a wide variety of skin, soft tissue and respiratory tract infections. These include strep throat and impetigo, but the most common illness caused by Strep A is scarlet fever, which is highly infections and has been spreading across the country.
But why are infections so awful this year? And what – if anything – can parents do about it?
Why is Strep A spreading?
Less mixing due to Covid could be part of the reason why hundreds of children are being diagnosed with Strep A-related illnesses this year. When social measures were put in place, the spread of Strep A was contained. Now, children who did not catch Strep A in 2020 or 2021 are being infected.
“It strikes me that as we are seeing with flu at the moment, lack of mixing in kids may have caused a drop in population-wide immunity that could increase transmission, particularly in school age children,” microbiologist Dr Simon Clarke, from the University of Reading, told Sky news.
What are the symptoms?
The best way to protect your kids is to know the symptoms and seek treatment quickly. It’s important to remember that Strep A causes a mild illness in the majority of children that can be easily treated with antibiotics. Symptoms include:
Advertisement
red and white patches in the throat
trouble swallowing
a headache
lower stomach pain
general discomfort, uneasiness, or ill feeling
loss of appetite
nausea
rash
“On darker skin, the rash can be more difficult to detect visually but will have a sandpapery feel,” Duncan Reid, pharmacist at Pharmacy2U told HuffPost UK.
Additionally, the British Islamic Medical Association explained that “the rash is more obvious in the groin/armpit area. Sometimes the flushed cheeks appear as ‘sunburned’ on darker skin with whiteness near the mouth”.
“In children with darker skin tones, the rash could be harder to spot as it may not appear red, but will be darker than normal skin,“ Dr Mabs Chowdhury, president of the British Association of Dermatologists added.
“The rash in all pigment types can have a sandpapery feel. The tongue can appear redder than normal with prominent white spots (sometimes called ‘strawberry tongue’).”
Advertisement
Where are the infections in the country?
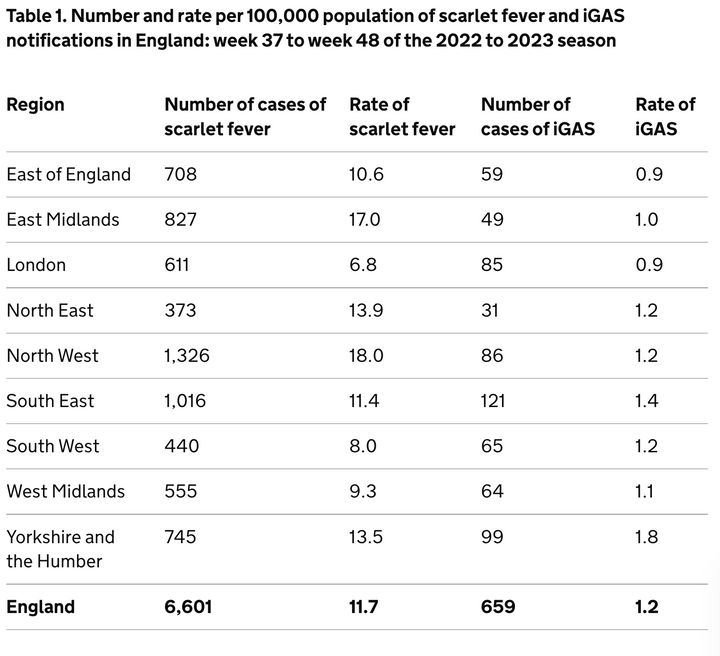
The latest available data shows that in England, there were 1,062 scarlet fever infection notifications received in week 48 (the week commencing November 28).
Currently, there are large concentrations of Strep A and associated scarlet fever cases in multiple parts of the UK, with the North West particularly impacted. The below data also shows incidences of invasive group A streptococcal infection (iGAS) – a rare but serious complication of Strep A, which can be life-threatening.
Number and rate per 100,000 population of scarlet fever and iGAS notifications in England: week 37 to week 48 of the 2022 to 2023 season.
How do parents feel?
Plenty of parents are beside themselves with worry right now as strep A continues to dominate the news. On social media and in private Whatsapp groups there’s been an outpouring of worry from parents, who are understandably on edge in case they miss the signs of illness that could progress to something far worse.
Advertisement
“I’m personally more worried about this than I was when Covid started,” said 35-year-old Emma Hawes from Wigan.
Hawes, who has a 13-year-old and eight-year-old, told HuffPost UK: “I am extremely anxious at the moment. I had no idea what the symptoms were so I’ve obviously been reading as much as I can.”
Diana Wilkinson, 45, has two children of primary school age. She told HuffPost UK: “I’m genuinely so worried about it. Every time I see the news it’s full of warnings of Strep A, and horrifically the number of fatalities is rising.
“Our school has been great at flagging concerns and sending out information about what to look out for, but with several cases already it feels very close to home.”
Is there an antibiotics shortage?
Some pharmacists are warning of a shortage of antibiotics – which hasn’t done much to quell concerns. However, the government has repeatedly denied it.
Advertisement
The National Pharmacy Association explained: “Pharmacies are having to work very hard to obtain stocks of these antibiotics and some lines are temporarily unavailable.
“We have been advised by wholesalers that most lines will be replenished soon, but we cannot say exactly when that will be.”
Leyla Hannabeck, CEO of the Association of Independent Multiple Pharmacies, claimed that authorities going on broadcast rounds saying there is supply is “misleading”.
“I want to reassure the public that pharmacies are doing everything we can to get hold of antibiotics and we are pushing the government to identify where the blockage is,” Hannabeck added.
Health secretary Steve Barclay said there was a “good supply” of penicillin, and that he had been reassured by medical suppliers. However, he said some GPs may experience shortages as stock is moved around to meet demand.
Advertisement
“Now, sometimes, GPs can have particular surges if they’ve got a lot of demand in an area, and that’s quite routine, we can move the stock around our depots,” he told Sky News.
Will schools close?
Currently, the Department for Education (DfE) has not updated its official advice to schools, but it is directing them to guidance from the UK Health Security Agency (UKHSA).
Parents were told to keep their children at home if they suspected that their children had Strep A, in a blog published by Dfe.
Education secretary Gillian Keegan said the department was “working closely” with the UKHSA and “monitoring the situation”, adding that the situation is “worrying”.
One school in Hull temporarily closed for a “deep clean” after several Strep A cases, but at the moment, schools on the whole are not being advised to close.
Advertisement
How do you catch Strep A?
Duncan Reid, pharmacist at Pharmacy2U explained: “Strep A is spread through contact with droplets from an infected person when they talk, cough or sneeze.”
“Some people can have the bacteria present in their body without feeling unwell or showing any symptoms of infections and while they can pass it on, the risk of spread is much greater when a person is unwell. It is still possible to infect others for up to three weeks.”
“Good hand and respiratory hygiene are important to top the spread of Strep A. By teaching your child how to wash their hands properly with soap for at least 20 seconds, using a tissue to catch coughs and sneezes, and keeping away from others when feeling unwell, they will be able to reduce the risk of picking up or spreading infections.”
When should parents contact their GP?
if you suspect your child has scarlet fever
your child is getting worse
your child is feeding or eating much less than normal
your child has had a dry nappy for 12 hours or more or shows other signs of dehydration
your baby is under 3 months and has a temperature of 38°C, or is older than 3 months and has a temperature of 39°C or higher
your baby feels hotter than usual when you touch their back or chest, or feels sweaty
your child is very tired or irritable
your child is having difficulty breathing – you may notice grunting noises or their tummy sucking under their ribs
there are pauses when your child breathes
your child’s skin, tongue or lips are blue
your child is floppy and will not wake up or stay awake.
Packing a nutritionally balanced lunch that your kids will actually eat can sometimes feel like a crapshoot – the second you think you have your lunch game on lock, that’s the day they’ll come home with the elaborate bento box you packed them still intact.
As parents, we feel responsible for our kids’ health and that understandably translates into a lot of stress over what they’re eating or not eating.
Advertisement
“Your job as a parent is to offer healthy, nutritious foods as often as possible, on a consistent schedule,” saidAubrey Phelps, a functional perinatal and paediatric nutritionist. “But it’s up to your child to decide what to do with them.”
The best way to grow a happy, healthy eater is to keep offering what you’d ideally want your child to eat – and don’t take it personally if they choose not to eat it. When it comes to school lunches, Phelps recommends keeping it simple: “Focusing on specific vitamins or minerals can miss the big picture,” she said.
If you use the following macronutrient formula to pack your kids’ lunch and vary the sources of each, you’re almost guaranteed to have a healthy, balanced meal that will keep them focused and energised at school.
The Formula
Advertisement
50% veggies and fruit
25% lean protein and healthy fats
25% starch or whole grains
+ fluids
The ideal school lunch formula is often referred to asthe plate method – a visual representation of what a well-rounded meal looks like.
“Every child needs a healthy balance of macronutrients (protein, carbs, fat) and vitamins and minerals,” Nicole Avena, a New York-based health psychologist and author ofWhat to Feed Your Baby and Toddler told HuffPost. “The plate method helps ensure that no one nutrient is overpowering the rest.”
If your child has a lunch that’s mostly carbs or whole grains and some protein, for instance, they’ll likely feel tired in the afternoon. Carbs not only make you sleepy due to their ability to increase tryptophan and serotonin levels in the body (both of which are sleep-inducing compounds), but they can quickly raise your blood sugar, and the subsequent drop can leave you feeling tired, Avena said. Even a larger portion of protein and smaller amount of carbs can make your child sleepy.
Advertisement
“Proteins and fats are often more difficult to digest than carbs and nutrients that come from fruits and vegetables,” Avena said. “This can potentially lead to fatigue, since your body needs to use up more energy during digestion.”
Making sure their lunchbox contains every element of this formula means your child will consume the balance of nutrients necessary to focus and enjoy their school day without feeling sluggish.
Let’s break down the formula.
Veggies And Fruit – 50%
Try: carrot sticks, bell pepper strips, grape tomatoes, cucumber, grapes, apple slices, watermelon, berries.
The biggest portion, or half of the lunchbox, should contain 2-3 different kinds of vegetables and fruit – preferably, two vegetables and one fruit, as children’s daily intake of vegetables tends to be lower than their fruit intake, according to a2019 review published in the American Journal of Lifestyle Medicine.
Claudia Totir via Getty Images
This is actually an example of what NOT to do. Don’t go heavier on fruits than vegetables, since most kids tend to eat more fruits anyway.
“Vegetables and fruit provide antioxidants to fight off disease, including vitamin A for skin and eye health, lutein for eye protection (from blue light) and vitamin C for immunity,” said Amy Shapiro, New York City-based registered dietitian and founder ofReal Nutrition.
Produce is also rich in water to keep kids hydrated, and contains fiber for sustained energy and improved digestion.
“Protein is the nutrient that takes the longest to digest, so having it as part of your child’s lunch will keep them full and their blood sugar stable,” Shapiro said.
Depending on the type of protein provided, it may also contain amino acids for growth and muscle repair, zinc for immunity, and iron and vitamin B12 for energy.
On to healthy fats: “Fat helps to keep you full, provides energy and allows for the bioavailability and absorption of many of the vitamins we eat through other foods,” Shapiro said. “By including fat in your child’s meals, you’ll help them stay full longer and be more energized.”
Enough fat is often cooked into your food or a part of the meal already, so it doesn’t necessarily need to be a separate addition, Shapiro said. (Eggs and nut butters, for example, offer a one-two punch of protein and healthy fats.)
“Carbohydrates are broken down into sugar in the body, providing energy for immediate use and reserves for later use,” Shapiro said. “Ideally, whole grains or whole wheat should be included, as they’re rich in nutrients, digest more slowly and are high in fiber to aid in balanced blood sugar and digestion.”
They also contain B vitamins, which are important for energy and metabolism.
But if your child isn’t the biggest fan of whole grains, don’t fret: “Vegetables and fruits also fit into the carbohydrate category, so you don’t always have to think about bread or grains if your child doesn’t like them,” Shapiro said.
Starchy vegetables and fruit include carrots, corn, potatoes, winter squash and bananas.
Advertisement
Fluids
Even just mild dehydration can cause a decline in cognitive function.
“Being dehydrated can affect reaction time, attention, memory and reasoning,” Avena said. “Children are potentially more at risk of dehydration because they’re more likely to be dependent on someone else for their fluid intake.”
Send your child to school with a large water bottle so they get enough fluids during the school day — and remind them to keep it at their desk.
“Out of sight equals out of mind,” Phelps said. “I also recommend a water bottle that’ll keep the water cold or room temp (however your child prefers) so they don’t get turned off by drinking warm water.”
It doesn’t have to be plain water, either: They might prefer fruit-infused, coconut or sparkling, or a different liquid entirely, like milk or 100% fruit or vegetable juice.
“If your kid really struggles to drink enough, consider sending hydrating foods,” Phelps said. “Soups, smoothies, juicy fruits like grapes and melon, bell peppers, even yogurt, are all hydrating options that can help keep kids on track.”
The easiest way to measure out lunchbox portions
Children are intuitive eaters – they’ll eat when they’re hungry and stop when they’re full, with the amount of lunch they eat fluctuating day-to-day – so there’s really no such thing as perfect portions to pack.
The easiest way to ensure you’re in the ballpark? Use your child’s hands as your guide.
Advertisement
Think of your child’s hands as a plate – palms up, pinkies together. Half of their “plate” (or one hand) should be veggies and fruits. The palm of the other hand protein, and fingers complex carbs.
“Using this method, the amounts needed change as your child grows (and so will their needed portion sizes),” Phelps said.
She’s also a fan of thebento box-style lunch containers, which are already sectioned off into child-friendly portions. You can fill one section with vegetables and fruit, one with protein and healthy fats and one with starch or whole grains sans guesswork. These ratios don’t necessarily need to be tweaked if your child has specific dietary needs.
“Appropriate substitutions are needed to ensure they have a filling and nourishing meal, regardless of the nutrition modifications that are needed,”Maya Feller, a Brooklyn-based registered dietitian, told HuffPost. The overall rule of thumb, however, generally stays the same.
Ratios and formulas should only be used as a guideline, not a hard rule, because children themselves should dictate how much they need to eat.
“If parents find their child is consistently eating 100% of foods packed throughout the day, it could be a sign they’re going through critical stages of development and require more energy,” Feller said.
It’s also important to keep in mind this is one meal out of their entire day — so if a lunchbox comes home practically full, it’s not game over. “We want to look at nutrition over the course of the day, not one meal,” Shapiro said.
When in doubt, you can check in with your kids: Ask how lunch was and make food and portion modifications based on the feedback given.
Remember: nutrition is cumulative
View your child’s nutrition over the course of a week, not a day – or a meal. “They’ll get what they need over time,” Shapiro said. “Some days are great and some days are off and it all balances out.”
Advertisement
The most important thing a parent can do is create a good relationship with food. That’s more important than creating the perfect lunch.
“Kids tend to be more black and white thinkers, so I don’t recommend focusing on ‘healthy’ or ‘unhealthy’ or ‘fun’ foods,” saidKrystyn Parks, a California-based paediatric registered dietitian. “All food is food. All foods have a purpose.”
Perfection isn’t the goal – setting routines that work for you and your child are.
“Find your own routine, get your kids involved in the choices and don’t measure yourself against another person,” Feller said. “No one day – or meal – is going to be perfect in terms of nutrition.”