But in a recent episode of his podcast Dr Karan Explores, surgeon Dr Karan Rajan spoke to doctors Dean and Ayesha Sherzai, neurologists and codirectors of the Brain Health and Alzheimer’s Prevention Programme at Loma Linda University Medical Centre, who shared that there may be other factors at play too.
Why might women have higher instances of dementia?
“We know that lipid metabolism and how women’s bodies respond to vascular risk factors, whether it’s an abnormal cholesterol panel or abnormal blood pressure, is different” than men’s, Dr Ayesha Sherzai said.
Advertisement
Cleveland Clinic says that women “face unique risks, largely due to differences in anatomy and hormones,” such as narrower blood vessels and fewer red blood cells, when it comes to heart issues.
“We also know that in the perimenopausal period, the woman’s body goes through a lot of physiological and neurological changes, because oestrogen is a very important factor in memory creation and in brain health,” the doctor added.
The combination of increased effects of vascular issues and the decline in oestrogen as women age “may increase the risk factors” of dementia for women, the expert says.
Any other reasons for the gender gap?
Harvard Health says that aside from the age difference, women are way more likely to develop Alzheimer’s than men. But they are not more likely to develop other kinds of dementia when you adjust for age.
Advertisement
Part of the reason for that may be that women are far more likely to experience autoimmune disorders than men.
That might be because women’s immune system is stronger, which may have the effect of creating more amyloid plaques in the body. These plaques have been linked to dementia.
The university’s site recommends taking aerobic exercise, like swimming, jogging, or dancing up for 30 minutes a day, at least five days a week, sleeping well, socialising, and eating well to mitigate the potential risks.
Before becoming a parent, I often heard from other mums about how self-aware you become when you have kids, but I never imagined how something as simple as a passing comment could ignite such deep reflection — and even make me fearful.
In early December, my daughter and I flew back to Colombia to visit my family. It was the kind of day I’ve come to cherish when raising a child abroad. But in the midst of all the warmth, I heard a phrase that made my heart sink.
Advertisement
“Don’t ask for too much; be grateful for what you have,” my grandmother said to my mum.
It wasn’t the first time I’d heard her say it. She had said it to me when I started many of my jobs, and she meant it with the best intentions of a caring grandma. In all of those instances, I didn’t think much of it. This time, however, it hit differently. This time, I pictured my 10-month-old daughter hearing those words one day, and the thought terrified me.
Beliefs like this one are not unique to my grandmother; many of us have them. However, working with female entrepreneurs to overcome financial trauma has taught me that phrases like these create a turmoil of mixed signals between pursuing what you want and staying where you are.
Why this phrase is so limiting
I’ve learned that every phrase reflects a belief system that makes sense for the season and context in which you grew up. For my grandmother, “don’t ask for too much” represented humility, gratitude and holding on to what she had accomplished with much effort. But it also discouraged her from taking further risks and continuing to nurture her ambition — and, consequently, my mum’s ambition.
Advertisement
I remember my mum once telling me how she had wanted to become a flight attendant when she was younger. Her face lit up when she talked about it.
Still, she never pursued it because, while deciding whether to stick with her current career — which offered security — or take a leap and pursue her dream, the phrase “don’t ask for too much; be grateful for what you have” echoed in her head.
How that phrase shaped me
I was only able to grasp the extent of how this phrase had shaped me when I left home at 19 years old and started living on my own. I started noticing the same patterns in my own life, and whenever I felt I wanted to reach for something different, aim higher, dream bigger, or ask for what I deserved, I had a little voice in the back of my mind that would make me hesitate to take the step. I’d feel as though I wasn’t being grateful enough or was asking for too much if, for instance, I wanted to ask for a raise.
Advertisement
This inner conflict only worsened when I started my business. I had to dream more significantly to create the kind of movement I wanted for female entrepreneurs and finances; I needed to ask for more. Although I had been very blessed to have already experienced things that nobody else in my social circle was experiencing — like traveling around the world — that inner hesitation made me question if I truly deserved and was capable of the career and lifestyle I was pursuing.
It wasn’t until much later — through my studies of financial trauma, therapy, self-reflection and the building of my frameworks for helping entrepreneurs achieve wealth — that I began to unpack how deeply ingrained those beliefs were.
Surrounding myself with ambitious, like-minded women also helped me see that those beliefs weren’t mine. They had been passed down, generation after generation, like an heirloom I never asked for.
Advertisement
Breaking the cycle for my daughter
Now, as a mum, I’m determined to rewrite what was once a subconscious narrative. I want my daughter to grow up with a mindset that supports her in her dreams and growth and encourages her to seek as many opportunities as she desires. I want her to believe — and genuinely know — that she can dream big, ask for what she wants and deserves, and take up space in any room she enters.
But breaking the cycle isn’t easy. It starts with unlearning my subconscious beliefs, so I don’t unintentionally pass them on to her. For instance, when she asks for something — whether it’s a new toy or a more significant goal down the road — resist the urge to say, “you don’t need that” or “you already have enough.” Instead, I try to understand her context, explore what she wants, and help her determine what makes sense in her environment.
It also means modelling what I preach. I can’t tell my daughter to be ambitious while shrugging off opportunities myself. So, I’ve made it a point to dream big and take risks, even when they scare me.
Did you know only 40% of Britons have read a book or listened to an audiobook in the past year?
Yup ― according to a recent YouGov poll, two-fifths of us didn’t engage with the hobby at all in the past 12 months, despite half of us buying a new book in that time.
The average Brit read or listened to three books last year, they add. A further 10% read between six and 10 books; 10% read between 10-20; and a tiny 4% tore through more than 50 titles.
Advertisement
Those numbers changed according to gender, age, and class.
Women are more likely to read than men
The research found that 66% of women have read or listened to a book in the last year, compared to just over half (53%) of men who said the same.
Of people who read in that period, women were more likely to read fiction for some or all of their titles (63%) than men (46%).
Though most people who read do so once a week, women were twice as likely as men (27% vs 13%) to read every day, too.
Advertisement
Additionally, women seem to get their books from a broader variety of sources: they’re almost twice as likely to have borrowed books from their family or friends than men (37% vs 19%) or from a library (24% vs 13%).
And women were likelier to buy second-hand books (46% vs 32%).
Of course, those weren’t the only differences in reading habits. 65% of people over 65 read or listened to a book in the last year compared to 53% of 18-24-year-olds.
Class seemed to have informed how much people read too; 66% of those in middle-class households had finished a title in the last year, compared to 52% of people in working-class households.
Advertisement
Why might men read less often than women?
Vox pointed out that an oft-repeated stat ― that “80% of women” buy all fiction units ― doesn’t seem to have a reliable, current source.
But lots of data suggest that men do read at least a little less often than women, and also read less fiction.
Writing for The Guardian, author of The Authority Gap, MA Sieghart, says her research found that men are far less likely to read a book they know is by a woman than women are to read a book they know is by a man OR a woman.
Advertisement
NPR found that by 2020, the majority of all newly published books ― both fiction and non-fiction ― began to be written by women, which might play a small role in the disparity.
With that said, contemporary hits are far from the only option for men (men had the biggest slice of the publishing pie for most of history), and even new titles are not monopolised by women.
Perhaps, as a GQ writer speculated, reading is seen as anti-“hustle culture” and against some ideas of masculinity; though as they added, “there’s no concrete answer.”
Cleveland Clinic explains that we “can’t prevent it because it’s your body’s way of keeping your vagina clean and healthy”.
The fluid helps to prevent us from infection and stops the area from drying out (which would leave it vulnerable to bacteria).
Advertisement
What’s considered a “normal” amount of discharge varies from person to person, but it’s usually nothing to worry about.
However, some colour, smell, or texture changes can indicate an infection.
What are the signs my discharge is abnormal?
According to the NHS, “normal” discharge is clear or white in colour. It shouldn’t have a strong smell, and should usually be slippery – but can be thicker and sticky.
Discharge that smells fishy can be a sign of bacterial vaginosis; thick and white cottage cheese-like discharge can reveal thrush.
Advertisement
Green, yellow or frothy discharge can be a sign of something called trichomoniasis ( a sexually transmitted parasite), while discharge that comes with pelvic pain or bleeding can be a sign of gonorrhoea or chlamydia.
Discharge that comes with blisters or sores can be a symptom of genital herpes.
Your discharge can be heavier when you’re sexually active, pregnant or on the contraceptive pill. It can even fluctuate throughout your menstrual cycle.
When should I see a doctor about my discharge?
You should see your GP if you notice changes to your discharge’s colour, smell, or texture.
You should also speak to a doctor if you notice more discharge than usual, if you feel sore or itchy, bleed between periods or after sex, get pain when peeing, or notice pain between your thighs and stomach.
Advertisement
Otherwise, though, discharge is completely normal ― avoid using perfumed gels or soaps in the area or wash inside your vagina (douching), as this can get rid of the protective effect that discharge offers.
In an Instagram Reel that’s been viewed over 70 million times, site user Hannah Stocking put a book above her loo’s cistern, placed a seat cover on the toilet, and walked out to her partner.
“I have to go,” he said forlornly; “I love you,” they both whispered as he entered the WC.
Arms on a clock span as he played games, scrolled, and generally hung out in there, pants around his ankles. He eventually emerges, bearded and disoriented.
Advertisement
“When your man goes to the bathroom,” the caption reads.
It’s not just an anecdotal thing or a funny post, though; according to a survey run by UK Bathrooms, men spend, on average, one hour and 35 minutes perched on the toilet each week compared to women’s 55 minutes.
Why?
It’s not usually stomach issues; or at least, it’s less likely to be that than it is for women.
Dr. Kyle Staller, a gastroenterologist, told Yahoo Life: “It’s true that men do spend longer in the toilet or on the toilet than women do, but in reality are much less likely to have bowel issues and chronic constipation than women are.”
A 2017 study from the University of Oxford and the University of Canberra found that not only are men more likely than women to scroll on the loo (20% vs 26.5%).
A YouGov study also found women feel more nervous about going number two in public loos, where lines are generally also longer than men’s.
But if we’re being real, I reckon we all know the true answer ― a lot of men admit to looking for a bit of an escape and some “me time” on the porcelain throne.
: “Now that I live with my girlfriend, I often use that alone time to plan dinners for the both of us and just generally take stock of the days ahead and what I’ve got going on.”
But doesn’t everyone like some me time?
Well, yes.
“I’ve had some clients tell me that the bathroom allows for the perfect escape from parenting duties,” Jonathan Alpert, a psychotherapist and author, told LiveScience.
Advertisement
“It can be a hideout for people because no one ever asks what you’re doing in there, even if you take a long time. It can truly be a safe place.”
That’s despite Office of National Statistics data that showed fathers of children aged five to 10 enjoyed five hours more leisure time than women per week, and “consistently took more leisure time than women regardless of how old the child in their household was.”
A 2023 Mumsnet post from a poster whose husband took several half-hour-long loo breaks daily reads, “The house would [be] chaos, the family wouldn’t eat and nothing would get done if I took 20 minutes out several times a day.”
Of course, if medical issues are to blame, ensure you see a doctor. And if it’s not a real cause of contention, hey ― scroll away.
Just don’t stay seated while, er, exposed for longer than five minutes (that can cause piles); and if you dash to the bog every time you need an escape, you might want to consider other, less pungent sources of “me time.”
Now, there’s another heart health reason to be wary of alcohol, particularly for women.
In new research involving 432,265 people — roughly 243,000 men and 189,000 women between 18 and 65 — experts discovered that women who had on average more than one alcoholic drink daily were at higher risk of developing coronary heart disease. The research was conducted by Kaiser Permanente Northern California.
Advertisement
Coronary heart disease, also referred to as coronary artery disease, is a condition in which the “major blood vessels that supply the heart (coronary arteries) struggle to send enough blood, oxygen and nutrients to the heart muscle,” according to the Mayo Clinic.
Symptoms include shortness of breath and chest pain. But for many people, a heart attack is the first noticeable sign of coronary heart disease.
Women who drink 8 or more alcoholic beverages each week are at higher risk of heart disease.
For the Kaiser Permanente study, participants reported their alcohol use between 2014 and 2015. In the four years that followed, researchers analysed their coronary heart disease incidence and found that 3,108 participants were diagnosed with the condition.
Those who had one to two drinks each week were categorised as having low alcohol consumption; three to seven drinks for women and three to 14 for men were categorised as moderate consumption; and 15 or more drinks for men and eight or more for women were categorised as high consumption.
Advertisement
While definitions of binge drinking vary, in this study, it was defined as having more than three drinks a day for women and more than four for men. Researchers noted whether participants had taken part in binge drinking in the past three months. People who do not drink were not included in the study.
Researchers found that drinking eight or more alcoholic beverages each week was linked to a 33% to 51% higher chance of developing coronary heart disease in young to middle-aged women when compared with women who drank less, according to the Kaiser Permanente Division of Research. Those most at risk, though, were women who took part in binge drinking, which was linked to a 68% higher chance of developing coronary heart disease.
Alcohol’s negative impact on heart health has to do with a few factors. “Alcohol has been shown to raise blood pressure and lead to metabolic changes that are associated with inflammation and obesity, both of which increase the risk for heart disease,” senior study author Stacy Sterling told the Kaiser Permanente Division of Research.
While the worst impact was seen in women, men who engaged in binge drinking were 33% more at risk of developing coronary heart disease compared with those who were moderate drinkers.
“Women also process alcohol differently than men due to biologic and physiologic differences, and this may contribute to the increased heart disease risk we found,” said Sterling. “It’s concerning because there has been an increasing prevalence of alcohol use among young and middle-aged women, including in the number of women who binge drink.”
Advertisement
This research is set to be presented at the American College of Cardiology’s Annual Scientific Session in early April, and it has not yet been peer-reviewed.
The Good Brigade via Getty Images
People, especially women, who took part in binge drinking were at high risk of developing coronary heart disease.
If you want to drink less, here are some expert-backed tips.
With emerging research like this, it’s no wonder that concepts like “mindful drinking” and “damp lifestyles” — both of which decentre drinking — are popular.
If you are looking to curb your drinking habits, it’s a good idea to know some of the U.S. government’s guidelines for moderate alcohol consumption. If you choose to drink, the guidelines recommend no more than one drink per day for women and two for men. Once you know the guidelines, you can track your consumption habits to determine how much you drink. (The amount that people actually drink is often underestimated.)
If you like to have a different beverage after work or to break up the week, you can make mocktails or purchase nonalcoholic beers, wine and spirits. “The quality of nonalcoholic drinks and beers are much better than they were in the past,” Vanessa Kennedy, the director of psychology at Driftwood Recovery in Texas, previously told HuffPost. Having these kinds of drinks at the ready can help you reduce the amount of alcohol you consume.
Advertisement
Experts say that it’s also helpful to track why you’re drinking. Are you doing it because you’re stressed, or because you’re bored? Once you determine the reason that you’re turning to booze, you can think of different things to fill that void.
“If you are saying, ‘Well, I just need this drink because I just need to relax’ … that alcohol itself isn’t actually what helps you relax,” registered dietitian Sumner Brooks previously told HuffPost. A bubble bath or workout class may help you relax more than a glass of wine.
Most importantly, if you are worried about your drinking habits or think they’re problematic, it’s important to seek support from an expert. You can find a therapist who’s trained in substance abuse to help you move forward.
A Conservative MP has criticised the government over its handling of the group known as the WASPIs, saying it “should be ashamed”.
Backbencher Tim Loughton called for action after a major report – released last week – found the government should compensate those women impacted by changes to the state pension age.
Advertisement
He told Times Radio “a lot of women” in the Waspi group – Women Against State Pension Inequality – have suffered” due to this incident.
The Waspi campaign is made up of women born in the 1950s who were impacted by increases to their state pension age (from 60 to 65) so it was equal with men’s.
The change happened between 2010 and 2018. Many say they were not adequately informed about the shift, and so ended up losing out on several years of their state pension.
According to Waspi, more than a quarter of a million women have died since the campaign began.
Loughton said: “A lot of women have suffered over a long period of time, and many of them have died in quite tragic circumstances, which is why we need recognition for what they’ve gone through.”
Advertisement
“I think they [the Department for Work and Pensions] should be ashamed. The government has got to take note,” the Tory MP – who used to co-chair an All-Party Parliamentary group on the issue – said.
“The Ombudsman clearly found the DWP were guilty of maladministration, that they’ve not properly communicated these changes with a great number of women.”
The Parliamentary and Health Service Ombudsman published its second report into the issue on Thursday, and found those affected were not adequately informed – and therefore need an apology and payouts.
But during Sunday morning media rounds, neither the Conservatives nor Labour committed to compensating those impacted.
Chancellor Jeremy Hunt said the issue was “genuinely more complicated” than other schemes were compensation was now being handed out, adding: “There’s no secret vault of money.”
Advertisement
Labour Party chair Anneliese Doddssaid, “those women deserve respect, that’s the most important [thing],” but did not make any promises.
Sign up and we’ll email you a daily dose of lifestyle stories, covering sex, relationships, health, wellness, money, and green living.
Successfully Signed Up!
Realness delivered to your inbox
By entering your email and clicking Sign Up, you’re agreeing to let us send you customized marketing messages about us and our advertising partners. You are also agreeing to our Terms of Service and Privacy Policy.
To take just one stunning example, the British Heart Foundation explains that women 50% more likely to be misdiagnosed when suffering from a heart attack than men.
Advertisement
Twice as many women as men die from the underlying cause of heart attacks too – coronary heart disease.
Meanwhile, erectile dysfunction (which affects 19% of men) is studied in research five times more often than PMS, (which affects 90% of women), according to ResearchGate.
And endometriosis – where tissue like those which line the womb are found outside of the organ – can cause fertility issues, pain, fatigue and heavy bleeding as well as wellbeing issues. It takes an average eight years to be diagnosed.
Much of the issues come down to a lack of research and funding into women’s health.
The first ever plan to reduce these inequalities was only introduced last year in the government’s Women’s Health Strategy. It’s a start, but the examples mentioned above show we are still a long way off gender health equality.
Advertisement
So, what would life look like if women had the same healthcare as men? Women’s intimate health brand INTIMA has produced a report imagining just that – and its findings are extraordinary.
1. Equal health would shrink the gender pay gap
The gender pay gap is an issue women still struggle with around the world. From November 22, the average woman in the UK is effectively working for free until the end of the year – that’s how large the discrepancy between women’s salaries and men’s salaries is.
The charity calls for more flexible working in an effort to improve women’s pay.
But it’s also worth recognising that health plays a large role, too. A whopping 89% of people experienced stress or anxiety in the workplace because of their period.
INTIMINA points to research dating back to 2015, which claimed women in the UK take 17 million sick days a year because of PMS. A third of women also take at least four sick days a year.
Advertisement
More than a third reported heavy menstrual bleeding too, which has been connected to higher unemployment and workplace absences.
Research from BUPA found a million women dropped out of work because of unmanaged menopause symptoms.
If these conditions were better researched, addressed earlier and talked about more openly, it could reduce absenteeism in the workplace, INTIMINA suggested. Flexible working would help deal with these conditions, too.
Advertisement
2. Economic boost
If there was no gender health gap, It could save £18 billion a year, according to INTIMINA.
That’s because endometriosis costs the economy £8.2 billon a year through treatment, loss of work and healthcare costs.
So it makes sense to invest in services to help treat these conditions.
And, according to the NHS Confederation, every pound invested in the NHS ends up giving £4 back to the economy by boosting productivity and workforce participation – truly, a win-win.
3. Boost for perinatal care
Healthcare professionals too often miss new mothers’ mental health struggles, the report revealed.
NHS England’s website also explains: “Perinatal mental health problems that are not treated effectively cost society £8.1 billion every year, with the annual cost to the NHS estimated at £1.2 billion.”
Suicide is the leading cause of maternal death during pregnancy and up to one year after it ends in the UK.
But as INTIMINA pointed out, many of the physical issues like incontinence or prolapse can be treated with early intervention and physiotherapy – which can help make new mothers’ lives a little easier.
Advertisement
Ariel Skelley via Getty Images
4. Orgasm gap? Eradicated
Research from 2018 suggests women in lesbian relationships orgasm 86% of the time, and women in straight relationships 65% of the time.
For men, it’s 95% of the time in straight relationships and 89% of the time for gay men – meaning there is an orgasm gap.
But, if women felt more comfortable getting to know their own bodies and speak to their doctors, INTIMINA suggested this would change.
Advertisement
Reduced pain, better mental health and better sex would all have knock-on effects for women’s relationships, too.
5. Women’s mental health improves
More research into conditions impacted by women – like PMS and Endometriosis – could offer a substantial boost to women’s mental health.
If endometriosis could be diagnosed after the first GP appointment – instead of after the average eight years – it would help relieve the 95% of patients who reported it had a negative impact on their wellbeing.
INTIMA claimed: “Earlier diagnosis and more effective treatments would help to reduce the mental health toll of menstrual and reproductive health issues. Symptoms would no longer be a barrier to living a full and well-rounded life.”
Advertisement
The brand suggested that, in turn, this would help reduce depression and anxiety among those who suffer.
I love my little nephew. He has a kid-sized broom that he uses to dance around in his diapers to Freddie Mercury songs as if it’s his microphone.
And I love my little niece, to whom “uppy” means both “pick me up” and “put me down,” and to whom “no” is a magical word for exercising newfound willpower.
Advertisement
I’m always happy to see them, and I have a great time learning from and with them about the world. But when they go home, and the house is so nice and quiet, I breathe a deep sigh of thanks: I get to give them back!
Then I can decide with my husband, Tim, to suddenly go out for dinner (without a diaper bag or babysitter), to go camping, or to visit a casino. We can go see some raucous band and stay out till 1am, or we can fall asleep on the couch watching TV and drinking wine, and wake up whenever we want.
I’m in the phase of life when so many people I know ache to become parents, but meanwhile, I love being child-free. This is, believe it or not, all thanks to my own mum, who also loved her child-free life before she had kids, and made sure to let me know that was OK.
My mum is a badass. She was a nerd growing up, just like me. And just like me, she wanted to travel and go to college, but she had very few financial resources.
Advertisement
So, one day, she joined the army as an interpreter. She went to a language institute and passed a Russian-language program that only a tiny portion of her incoming class passed, and then flew to Germany to work on a mountaintop compound. She was one of three women in a company of 300 men listening to German and Russian soldiers on the radio, translating it all into English for Army intelligence.
That’s where she met my dad. They got married and travelled, came back stateside, and went to college. Roughly eight years later, they had me.
It’s no wonder, then, that when my mum asked me what I wanted from my life as I was having a teenage existential meltdown, I said: “I just want to have an extraordinary life.”
I wanted to travel, take risks, get into trouble, have adventures, go to college and, eventually, make what I hoped would be a positive difference in the world.
I was inspired by my mum’s own life. And at that time in my world, like her, I felt limited only by money, as I had all the other great propulsive forces of youth, like energy, recklessness and idealism. Plus, after my parents’ divorce, my mum, my brother and I lived in my grandmother’s attic, and space was a little tight.
Advertisement
I wanted to explode outward into newness. So when I did move out of the house with my first boyfriend, at about age 20, and my period was late one month, that potential pregnancy felt to me like a very bad thing – not a boon.
I hadn’t travelled.
I hadn’t gone to college, or had any adventures.
I hadn’t taken any big risks.
I sure hadn’t made a difference in the world.
Nick was a nice boyfriend, and he told me he’d get on board with whatever path I wanted to choose: get married and have the baby, have the baby and not get married, put the baby up for adoption, or get an abortion.
I thought about it for a few days and tried on all of these options in my mind. But after much mulling, the only way that felt right was to go on with my original plan of having a wild and free life. I didn’t want a baby. I didn’t want to be pregnant.
I felt like I was about to get stuck in my hometown for the next few decades, changing diapers and picking out public schools.
I decided I would get an abortion on the same day my period came back of its own volition, and I heaved a mental sigh of relief.
Advertisement
However, I was very aware that I had dodged a big baby-sized bullet, despite all of my birth control efforts from the age of 15 onward. And I decided, if I was not to become a mum, that I wanted to be able to have sex like a man, with fewer consequences in the reproductive department.
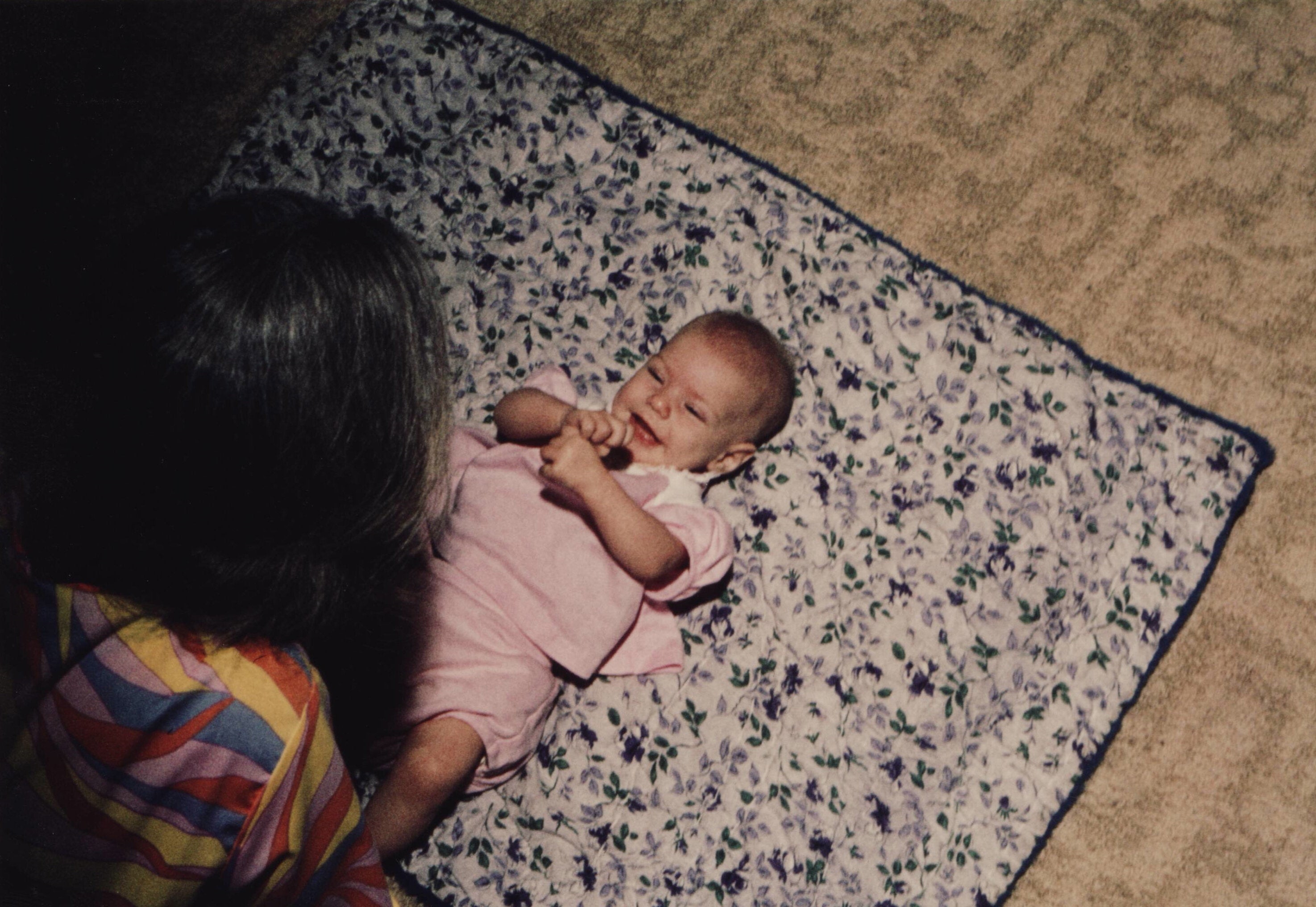
Courtesy of Lydia Paar
The author, in her early 30s, with her mom in Arizona.
I was able to admit to myself for the first time that I knew I did not ever want to have kids – at least not in any traditional biological sense. If I ever changed my mind about mothering, well, there are millions of kids in the world needing homes.
So, I went and talked to the only person I felt might really understand my need to not mother: my mother.
My mum did something very important for me as I was growing up: she’d told me about some of her experiences in the sex realm, helped me to understand what I was feeling when these experiences started to arise for me, and answered all my questions about how this weird and impactful part of life worked.
Advertisement
Because of this open channel of communication, I knew that my grandmother had flown my mum to Japan in the ’60s for an abortion when she was 18, after American doctors they’d consulted said she “didn’t look sad enough” for a procedure here.
And just as I’d hoped she would, my mum helped me. She offered to take me to get an intrauterine device. I said I’d prefer to just have my tubes tied and be done with it, having already heard my fair share of IUD health horror stories (including hers).
And instead of telling me to “just wait and see” or that I would “probably change my mind” like so many other people have, she called around and got me into an abortion clinic, where I sat down with a counsellor and earnestly explained my desire never to have children. Within a week or two, I had an outpatient tubal ligation procedure.
Looking back now, I realise it must have taken my mum a lot of searching to find a doctor willing to perform this on such a young woman with no previous children; most doctors wouldn’t have, whether out of fear of being sued if I did “change my mind,” or because so many people still believe that all women inherently want or ought to have children.
I also know now, having had my own health care plans and understanding what “elective surgery” means, that when my mum said she had “wrangled things out with our health plan,” she meant she had in fact quietly paid for this surgery for me out of pocket.
Advertisement
So here I am, child-free at 40 and at the doorstep of menopause, remembering, with gratitude, this generous gift. I also remember those other voices:
“You might change your mind.”
“You’re just not ready yet.”
“Your biological clock will kick in someday.”
These are sentiments that have floated around me for years, before and after my tubal, not only from the popular media but from people I’ve loved and trusted. And these are mythologies that surround every woman on the planet, every day: the idea that we are born and built to breed.
“Womanhood is not synonymous with motherhood. For many of us, our truest selves are the selves without progeny.”
We are, as an American culture at least, very much in midprocess of correcting this idea. Womanhood is not synonymous with motherhood. For many of us, our truest selves are the selves without progeny.
And when people, often women, ask me how I feel about things now, I tell them wholeheartedly that I’ve never regretted my decision to amend my reproductive capacities – not once. (I’ve even recommended the procedure to interested parties.) But it’s also important to acknowledge that if I did have regret, it would have been my own choice to regret – not anyone else’s. And that kind of regret, born of agency, is still good; it would have been mine to own.
Advertisement
Needless to say, it’s since become important to me that other women know this “child-free by choice” option is viable from early on in our lives.
I would have been a bad mum at 20: resentful and risky and selfish. I’d still be a mostly bad mum – a little more risk-averse, but covetous of my time alone, my mobility, and my ability to have sex anytime I want without period planning, birth control side effects, and potentially life-changing consequences. I’ve gotten to move over 25 times in the past two decades, meet a ton of people, see and do crazy things, and go to college – a lot.
I’ve been able to reallocate my energy to get really good at other things besides mothering. Not that I buy into the “either-or” myth of motherhood; there are many amazing women who can manage an impressive amount of autonomy, professionalism and wildness while still doing right by their children. It’s just that I knew I couldn’t – and I didn’t want to anyway.
And it’s because people listened to me – my mum and the counsellors and doctors at Oregon’s Lovejoy Surgicenter – that I was able to live the life I wanted to live.
So my takeaway here, besides the closely related “vote pro-choice” sentiment, is that when someone, especially a woman, says, “I don’t think parenthood is for me,” we need to honour and respect them in the same way we would an aspiring parent. Both choices are equally natural, equally potent and equally rich with possibility.
Advertisement
Doctors, support women in permanent birth control when they ask for it. Friends and family, believe what women tell you about their bodies.
Then there remains just this little bonus takeaway: We should remember to enjoy, and to spoil, our nieces and nephews, at least a bit, before we give them back to their parents, who chose the hard work that parenthood entails.
Lydia Paar is an essayist and fiction writer. Her essay “Erasure” was of notable mention in the 2022 “Best American Essays” collection, and was the 2020 winner of North American Review’s Terry Tempest Williams Creative Nonfiction Prize. The New England Review nominated her as a finalist for its 2021 Award for Emerging Writers, and her works have been showcased in outlets such as Literary Hub, The Missouri Review, Essay Daily, Witness, Hayden’s Ferry Review and others. The recipient of an MFA from Washington University in St. Louis and a master’s from Northern Arizona University, Paar is also a former recipient of a Frederick & Frances Sommer Fellowship and of a Millay Arts residency. She currently co-edits for the NOMADartx Review and teaches writing at the University of Arizona. Her first full-length essay collection, “The Entrance Is the Exit: Essays on Escape,” is forthcoming from the University of Georgia Press. She can be reached there or at www.lydiapaar.com.
Do you have a compelling personal story you’d like to see published on HuffPost? Find out what we’re looking for here and send us a pitch.