On January 22, 1973, the US Supreme Court affirmed in a 7-2 decision the legality of women’s right to have an abortion under the 14th Amendment.
Today, about one in four pregnancy-capable people in the US have had an abortion, and the risk of complications from an in-clinic procedure is extremely low. But before it was guaranteed as a constitutional right, seeking an abortion was a harrowing, potentially life-threatening endeavour.
Advertisement
While some women saved up the cash and sometimes travelled hundreds of miles to find qualified medical providers willing to risk their livelihood by operating on patients, others settled for providers lacking the qualifications and skills to perform induced abortions. And even more desperate people attempted their own abortions.
The outcome of these back-alley procedures or at-home coat-hanger abortions was often devastating, leading to maternal death or lifelong injury. (Complications from unsafe abortions include infection, incomplete abortions, haemorrhaging, uterine perforation and damage to the genital tract or internal organs, according to the World Health Organisation.)
Advertisement
Because these stories were so traumatic – and because the stigma surrounding abortion was even greater in those pre-Roe v. Wade years – many women remained silent about their experiences.
Now, as the US Supreme Court seems poised to overturn the Roe v. Wade decision, it’s worth revisiting their stories to understand what abortion was like in the decades before it was legalised.
Advertisement
HuffPost US recently spoke to eight people who shared experiences of relatives – great-grandmas, grandmas, mothers and aunts – who sought abortions in pre-Roe v. Wade America. Many were already mothers, struggling to conceptualise raising one more child in poverty or, in some cases, with an abusive spouse.
In one story that differs from the rest, a reader shares how her great-grandma, the wife of a well-to-do dentist, was able to obtain a safe abortion in a doctor’s office with little fuss; the story illustrates how white, middle-class and upper-class women have always had an easier time accessing safer abortion options. (As many have noted, women of colour will be disproportionately affected if Roe v. Wade is overturned.)
Below, read all eight stories, which have been edited lightly for clarity, style and length.
“My maternal grandparents married in 1934. By the time my mother was born, it was clear my grandpa was a monster. Violent and cruel, he beat my grandma with a metal lunchbox. When mom was just a few months old, he threw her against a wall. My grandmother fled.
Advertisement
She discovered she was pregnant again. To induce an abortion, she drank a bottle of Lysol. You can Google ‘Lysol abortion’ and see ads from that time that suggested a woman could use Lysol to ‘correct your mistake.’ The ads are quite chilling, their meaning vague and without instructions.
It took my grandma 29 hours to die in her parent’s home; they were helpless to end the agony. Living in a logging village in winter, there was no hospital or way to travel to the city.
My mother always felt responsible for her mother’s so-called ‘suicide,’ as children do. Doing genealogy research, I uncovered the full story when my mother was in her late 60s, but her life was already written and the truth brought no comfort. I sometimes think I should never have done the research. There are four generations impacted by this one attempted abortion. We can never really know how lives would be different if she had lived. But I do know my mother’s life was forged by that event, she was an orphan, hidden from her father, never knowing why she’d been abandoned.” – Chuck M., 62, from Washington state

“My mother was a 16-year-old in 1970 when she became pregnant as a result of sexual assault. She was living with my grandparents in Southern California, and abortion was not legal at that time. My grandparents were not in a position to get over the border into Mexico to have the procedure done, and they didn’t have access to a safe place to have the procedure done, either. Rather than risking my mother in a back-alley abortion, my grandmother assisted my mother in inducing a miscarriage. My grandmother had my mother sit in steaming hot baths for hours. My mother ingested medications that were considered dangerous to a fetus. They did everything short of physically harming my mother, though my mother did tell me that she was so desperate to end the pregnancy that she considered throwing herself off a high platform or down the stairs.
They managed to successfully induce a miscarriage, and my mother was taken to the local hospital to deal with the effects of the miscarriage and for a dilation and curettage. That worked, but her young body and mental health were not OK. Though my grandmother’s and mother’s intentions were to do something safer than a back-alley abortion, my mother was still at risk of potential harm from the various medications she took. And the foetus would also have been at risk for birth defects and other issues if the medications had not succeeded in a successful miscarriage. It was still dangerous.
My mother told me once that Roe was the single most important law that passed in her lifetime. That she was relieved that other women and people with a uterus would not have to suffer the same circumstances she did. If she were alive today, she would be absolutely shattered.” – Sara from New York
“My aunt Judith was just 17 in 1964 when she became pregnant after being raped on a study date at a so-called friend’s house. She was horrified to find out she was pregnant; she was on her way to college in the fall, and a baby wasn’t in her plans yet. Her doctor suggested a girls home out of town where she could stay until the baby was born and then give it up for adoption; it was her only choice since abortion was illegal.
Judith had tried all the old wives’ tales, jumping backward a dozen times at dusk and even drinking a tea that made her deathly ill just to lose the pregnancy naturally, but nothing worked. A friend of hers, Arbie, who was two years older, had been in Judith’s shoes and had taken care of her ‘dilemma’ herself.
In that summer of 1964, Judith chose to use a metal coat hanger, thinking it would be over quickly and no one would ever know. Her end result was far more than she had ever anticipated, with excessive bleeding and infection that led to a partial hysterectomy and the inability to ever carry a child. She spent nearly a month in the hospital. Her mother found out and never looked at her the same, although she did keep [Judith’s abortion attempt] from Judith’s father, knowing he would have kicked her out and pulled her college tuition. The family was hush-hush about everything, given the era everything took place.
Judith went on to graduate college top of her class to become the first female doctor of psychology in the family. From the outside looking in, her life was perfect: the house, her own office, nice car, all the material things one could ever hope to have, but she had developed a serious drinking problem and her life behind closed doors was, as she once said, ‘exactly what you’d think hell on earth would be.’
Advertisement
I was born in ’72, her only niece at the time, and she doted over me constantly every chance she had. I never suspected anything was ever wrong, although I did always wonder why Auntie Judy had such sad eyes; it wasn’t until puberty hit for me that she warned me of the dangers of having ‘that time’ and told me her story. She explained there were no real options in ’64 but said that because of Roe v. Wade in ’73, I would have more options than she had ever had.
Her desire to be able to carry a child, to be the mother she had always dreamed of, haunted her every waking hour and her dreams, and she was never able to get away from it. In 1984, just a week shy of her 37th birthday, my Auntie Judy hung herself in her attic; the pain and anguish had finally won the battle. Her note was a short novel, telling her story. I was only 12 and was told I wasn’t old enough to read it or understand it, but I didn’t listen. I sneaked and read it, and now I can remember every word, and her pain, longing and anger still haunt me to this very day.” – AJ, 50, from Louisiana

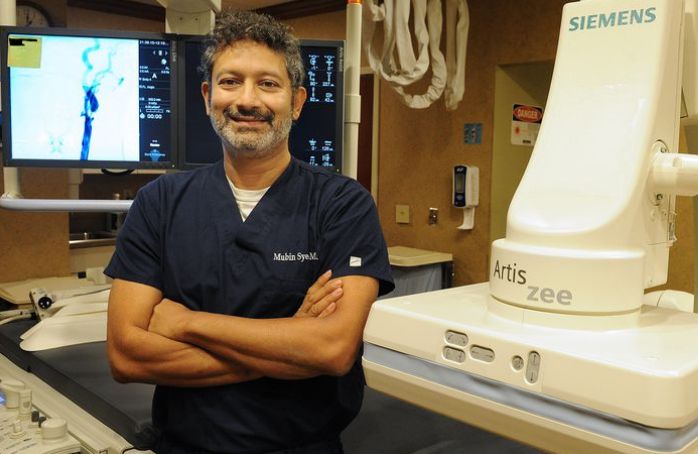
Jared Milrad/Canva
“Like most kids raised by a single mother, I’ve always thought of my mom, Jan, as courageous, resilient and strong. Growing up, she commuted nearly two hours each day ― every day ― to work a low-paying job as a secretary so that my brother and I could have a better future. Despite all that she went through, my mom never gave up and ensured that my brother and I could get the best education and have more opportunities than she did.
But it wasn’t until I was in my 20s that I realised how truly incredible my mom is. One day, my mom shared that she was around my age when she had two abortions. This was 1968-69, when abortion was still illegal in the U.S. and my mom was 26 or 27 years old.
My mom told me that she had her first abortion during this time while dating a much older man. The pregnancy was very unexpected, and because my mom was struggling to make ends meet and didn’t have much support at all, she made the wrenching decision to abort the pregnancy. Because abortion was illegal in the States, the man found a doctor for her in Puerto Rico and agreed to pay for the procedure, so my mom went with my grandma to have it done. They traveled to San Juan and then traveled a bit outside of the city. My mom expected the procedure to be done with anaesthesia, but – horrifyingly – it wasn’t.
‘The abortion was done by a butcher and my mother heard me screaming,’ my mom recalled. ‘I didn’t know that they weren’t going to give me anaesthesia. It lasted for only 20 or 30 minutes, but it seemed like a lifetime. When we got back to the hotel in San Juan, I was in such pain. Then, when I was back in New York City in A&P Grocery a few days later, I noticed that I was bleeding ― haemorrhaging.’
My grandma immediately called a gynaecologist and arranged to have my mom treated in the ER at Lenox Hill Hospital, where they didn’t tell the doctors that the bleeding was caused by an abortion out of fear because the procedure was still illegal. My mom was lucky to survive.” – Jared Milrad, 38
“Today, the majority of women who seek a legal abortion are already mothers. Let me share a pre-Roe horror story about my Italian, Catholic grandmother Mary, whom I never had the blessing to know.
Apparently, on her deathbed in 1943, Mary asked her sister-in-law Florence, who was childless, to take care of her only daughter, but the shameful secret had to be kept. My mom was forbidden to ask questions about her mother or her death. She learned the truth when she was in her 50s from me after years of research.
I was in my 20s when I first began to put together the pieces of a story that just didn’t make sense: a 34-year-old mother of three young children who is hemorrhaging but refuses to go to the hospital. Even the death certificate corroborates the secret. Cause of death: carcinoma of the cervix. But cervical cancer does not generally cause women to bleed to death.
Advertisement
Then, one day in the mid-’70s, we were talking about the Roe decision, and Florence, the woman I knew as my grandmother, let it slip that she had to lend $250 (an enormity in 1943) to one of her brothers because someone needed an abortion. I was stunned; I finally connected the dots. In a typically large Italian Catholic family, Florence had many sisters but only two brothers. One of them, it turns out, was my biological grandfather.
Grandma Mary already had three children she loved: two boys and the middle child, my mom Nancy. With an unemployed husband, a fourth child would plunge the family into poverty.
So the decision was not made lightly, but something went horribly wrong. Mary was just 34 years old and was more afraid of the law (and the judgment of the Catholic church) than she was of dying and leaving her children motherless.” – Lori Bores from New York
“Great-Grandma Selma Rosenthal (born 1878) was a career woman. Graduating from college in 1901, she was homely and smart, two things that did not make her particularly attractive to suitors of the era. Knowing this, she focused on having a successful career. She was by all accounts very funny, with a wonderful voice and an active circle of friends. She had no expectation that marriage or family were in the cards for her, and she had made peace with that idea.
That all changed when she met Sidney Rauh, a dentist from Cincinnati from a well-off family. It was the 1910s, and she was well into her 30s. Sidney was equally unattractive and clever, and a confirmed bachelor. He had no interest in marrying a girl for her looks but wanted to find someone he could love for her mind. When they met, it was love at first sight, and given their advanced ages, they decided to marry as soon as possible.
Selma quickly became pregnant, only to miscarry the first Christmas they spent together as a married couple. Two daughters quickly followed in 1916 and 1919, but Selma was terribly sick with her second pregnancy and she barely survived childbirth. Her doctor told her, in no uncertain terms, that if she was to get pregnant again and attempt to see it to term, she would die. She promised she would be careful.
A few years later, when she realised she was pregnant, she went to her doctor. The doctor advised her that she had to have an abortion. Sometime later, the doctor performed an abortion in his office, no fuss, no muss. But Selma was a well-off wife of a successful dentist with status in the community. It never occurred to her that what she was doing was illegal or in any way wrong. It was a decision between her, her doctor, and Sidney, and she did what was best for her family and health.
Selma died in 1948 at the age of 62 of a heart attack, having spent time not just with her daughters, but also with her granddaughters, who were five and three at the time of her death.
Great-Grandma was a suffragette and strived for women’s rights. Women’s rights and bodily autonomy were key issues in my family, but I suspect the story would not have been noteworthy had it not been for the fact that abortion became the issue it was later on. My mother and grandmother shared with me how hard things like birth control had been to get in their era, and my mother shared with me the fact that she got a (legal) abortion for family planning reasons. For us, it was just part of normal conversation.” – Kate, 50, from New York

Stephanie Voltolin/Canva
“I was born in the 1960s and grew up in a very conservative Catholic family. Nonetheless, my traditional housewife mother was ardently pro-choice. She even took one of my friends to get an abortion in the 1980s because my friend couldn’t tell her family she was pregnant.
Advertisement
Shortly after my paternal grandmother died, when I was a college freshman, my mother frankly told me during a conversation about choice, ‘Your grandmother had a back-alley abortion and almost bled to death.’
My grandmother found herself – in the early 1940s before birth control or abortion were legal – pregnant and divorced from her second husband, who turned out to be horribly abusive. She decided to leave before he began abusing her three children from her first marriage. Like most women of her day, she had no college education or career to support herself and her children. And, like most women who get abortions, she could barely support the children she had. She ended up having to go live with her parents, who were Italian immigrants.
Faced with being twice divorced and pregnant, my grandmother sought an abortion. Because they were illegal, she had to trust a back-alley ‘doctor,’ who punctured her uterus in the process. She left the procedure, collapsed in the street from the blood loss, and had to be taken to the hospital. An emergency hysterectomy saved her life.
She was an amazing mother and grandmother, and although she died almost 40 years ago, I still become emotional when I think about what a loss I would have suffered had she died from that botched abortion.
The rest of the family never knew. I am telling her story now in the same way that we disclosed our sexual trauma during the Me Too movement to educate others. Legal and safe abortion is critical to women’s reproductive rights as American citizens, and we cannot allow them to expire.” – Stephanie Voltolin

“My great-grandmother died from a botched, illegal abortion in the mid-1930s in Chicago, leaving my grandmother (2 years old) and her sister (4 years old) without a mother. When my great-grandfather remarried, his new wife already had kids of her own and didn’t want to take care of two more. My grandmother and her sister were thrown out of the house and bounced around to different aunts and uncles.
For much of my grandmother’s life, she was told that her mother died of a pregnancy complication due to an ectopic pregnancy. Later, when my grandma was a teenager, her aunt told her the truth: that her mother had died from a botched, illegal abortion.
My grandmother shared her story with me in 2012 when I was 25. We were having an early lunch. I remember she asked me if I wanted a glass of wine, which was odd for her in the middle of the day. We were talking about something else entirely and she said, ‘my mother died of a botched, illegal abortion,’ almost out of the blue, and her story just unfurled from there.
I honestly didn’t think too much about what my grandmother shared. I didn’t think her story was shocking or novel, maybe because abortion had been legal in all 50 states for my whole life. I assumed everyone else in our family knew, so I didn’t think to say anything.
A couple years later, I was catching up with my parents and one of them said, ‘Did you know Great-Grandma Sally died from a botched illegal abortion?’ That’s when I realised my grandma was nervous when she shared her mother’s cause of death with me. She was holding on to this family history and likely carrying with her the shame and stigma or the ‘don’t talk about it’ attitude of her family. It was an ‘aha’ moment for me – a real understanding that likely everyone has a family abortion story, whether they know it or not.
Advertisement
Now our family has a deep understanding that when abortion is legal, abortion is safe. And we know in the decades before Roe v. Wade was decided, people like my great-grandmother were desperate to receive the care they needed.” – Amy Handler, 35, from Oregon