Employees undergoing fertility treatment could soon be entitled to statutory time off work, under a proposed law being brought before parliament.
The law suggests that fertility appointments should be treated in the same way as antenatal appointments during pregnancy.
Advertisement
NHS England and NHS Improvement have already recently given roughly 8,000 of their staff the right to three days off a year specifically for fertility treatment, The Mail on Sunday reports. (Though it’s worth noting that free IVF treatment under the NHS has faced huge cut backs in recent years.)
Under the latest bill, proposed by Tory MP Nickie Aiken, all companies would have to give both women and their partners time off for fertility treatment. It’s hoped the change will help those who may currently be going through multiple rounds of tough IVF treatments in secret.
“Undergoing treatment while juggling a career is very tough,” Aiken said. “Many people feel they cannot tell their employer for fear of being overlooked for a promotion or being made redundant.”
Why is this new proposed law so important for hopeful parents?
Becky Kearns, Co-Founder of Fertility Matters At Work, tells HuffPost UK this law is potentially game-changing, because it gives people “permission to talk to their employer about going through treatment (if they choose to) rather than feeling like they have to hide it”.
Advertisement
“We know from our research that 61.1% did not feel confident talking to their employer about trying for a baby,” she explains.
“Many fear that there will be an impact to their career in asking for time off to attend appointments and so a law in place to give a statutory right and protection against unfair treatment will help them to know that this is recognised by their employer.”
She adds that IVF is often seen as a ‘lifestyle choice’ rather than a treatment for a medical condition – though the World Health Organisation describes infertility as a “disease of the reproductive system”. The proposed law would help to right this wrong.
How will this benefit people who are having IVF?
Kearns believe this will benefit hopeful parents as IVF is a gruelling process over the course of a number of weeks involving numerous, frequent and unpredictable appointments. “From my own personal experience, taking time off for fertility appointments felt very different to when I finally became pregnant and was ‘allowed’ by law the right to attend antenatal appointments,” she says.
“It not being recognised or even allowed within many organisations creates additional stress and burden on top of an already emotionally draining process. This law would mean that over time fertility appointments would also be expected, accepted and acknowledged as a statutory right.”
Advertisement
What are some of the work challenges women face when undergoing fertility treatment?
When going through IVF or other fertility treatments, women face “a very real fear of not being seen as committed to their jobs, of being overlooked for promotion or even selected for redundancy if their employer knows,” Kearns says.
“It’s also a hugely personal experience, one that still often has stigma and shame attached to it,” she adds.
“Planning is hugely difficult as it often depends on how your body responds to treatment and when your period starts as to when treatment can begin, the appointments can be every other day and sometimes at late notice depending on blood test and scan results.”
In a 2020 survey by the community interest company, 83% of respondents said Covid (and working from home) had made it easier to plan and squeeze in fertility treatments. But now most of us have returned to the workplace – at least some of the week – things will get harder again.
“There’s the physical challenges of the hormones that are injected, also the challenge of finding an appropriate place to administer injections and pessaries whilst at work, one woman told us she had to hide her in a sandwich box in a fridge,” Kearns explains.
Advertisement
“Financial worries are huge too with the cost of treatment often running into the thousands, another stress when you need to take time off work – some are told to use annual leave or unpaid leave, we found that 69.5% took sick leave during treatment.
“Most predominantly is the mental health challenge, we found that 68% felt their treatment had a significant impact on their mental and emotional wellbeing, having to hide appointments and the huge grief that this process brings about can make it even more of a challenge, to the extent that 36% considered leaving their employment due to treatment.”
Let’s hope the bill marks the start of the change that’s needed.
An STI which is virtually unknown to the public is likely to be found in Black, Asian and other minority women more frequently, according to new research.
While more common than other sexually transmitted infections such as gonorrhoea, the virus Trichomonas vaginalis (TV) is largely not known about to large swathes of people.
Advertisement
But new research shows that it is more common among ethnic minority women and can appear with common symptoms or asymptomatically.
Without treatment, the condition can have serious consequences, increasing the likelihood of HIV and pregnancy complications, which is why it’s important we get clued up on it.
The research, presented by Preventx at the British Association for Sexual Health and HIV annual conference, found that TV is also more common among heterosexual people. They studied 8,676 women from six English local authority areas who had completed remote STI tests.
While women of colour were most likely to be affected, Black women were particularly found to be at risk.
Advertisement
In the study, they found that 5.2% of women from Black, Caribbean and African heritage who had vaginal discharge – a common symptom of the infection – ended up testing positive for TV.
For all other women, the risk of having and displaying signs of the condition were 3.5%, with white women facing lower chances, at 3.4%.
Even in Black women who did not show any symptoms, the chances of TV remained higher among them, with a positivity rate more than twice as high as for white women. For Black women, this figure was eight times more likely, whereas for white women it was twice.
But it might not be genetic differences that predispose more women of colour to the condition than white women – it could be to do with levels of social deprivation.
For the first time, scientists also considered the relationship with poverty and rates of TV.
They found that the highest levels of TV were found in disadvantaged areas, with 5.9% of women in the most deprived neighbourhoods (in which women of colour are more likely to reside) testing positive for TV. In affluent areas, this number is at 1.4%.
Advertisement
Dr John White, medical director at Preventx and consultant physician in sexual health commented on the study, saying: “Trichomoniasis is a relatively unknown STI among the general population, but it can cause significant pain and discomfort. I know from the patients in my care that it can also cause a lot of emotional distress for the person infected too.
“Women, in particular, can remain infected for years – and their distressing symptoms are often misdiagnosed or dismissed. If untreated, TV can also increase the chance of acquiring HIV in at-risk communities, as well as cause complications in pregnancy.”
Scientists hope more research and testing is done to understand and treat the condition.
Dr White added: “Our new data shows worryingly high positivity rates, with certain communities more affected than others. As TV can easily be diagnosed with remote NAAT tests, it is vital that more high-quality TV testing is carried out across the UK, helping us to understand more about the distribution of this infection.
“This will allow us to address the consequences of undiagnosed TV and reduce transmission.”
What is TV and what are the symptoms?
TV can affect both men and women. According to the NHS, symptoms of trichomoniasis usually develop within a month of infection. However, up to half of all people will not develop any symptoms (though they can still pass the infection on to others).
The symptoms of trichomoniasis are similar to those of many other STIs so it can sometimes be difficult to diagnose.
How much sleep are you getting? Judging by how you’re feeling, you’d probably say ‘not enough’.
Many of us dealing with the drudgery of the day often don’t feel very well rested and are likely to wish for more snoozing time. But actually, we might be sleeping too much already, depending on our age.
Advertisement
The ideal amount isn’t actually eight hours for those over 38 years old, according to scientists who conducted a major new study.
The University of Cambridge and Shanghai’s Fudan University examined the sleeping habits of nearly 500,000 adults aged between 38 and 73 and found that the ideal amount of sleep may be seven hours.
Advertisement
Participants were tested on their cognitive abilities and asked about their sleeping patterns, wellbeing, and mental health.
Researchers also sourced brain-imaging and genetic data for up to 40,000 participants in the study to get a better insight into their wellbeing.
Advertisement
Interestingly, they found that getting too much sleep and not enough has the same consequences. While traditionally, we’re told to get eight hours, scientists found that this amount, or any more (or less than seven) have a negative effect on our bodies as we age.
They found that too much sleep and not enough both had a detrimental effect, causing mental health issues and ‘worse cognitive performance’.
The study also showed that being consistent is key, so getting six hours one day and then nine the next can still leave you feeling groggy and tired.
So, why exactly do we feel a brain fog when we wake up some mornings?
Advertisement
Researchers say that it could be due to slow-wave deep sleep being disrupted during shorter bouts of slumber. This means the brain doesn’t have enough time to clear out the toxins.
Not only is getting the right amount of sleep better for your overall wellbeing, it’s good for our memories. That’s because scientists found that the hippocampus – the memory centre – is also affected by a lack of or excess of sleep.
So the older you get, the more you might want to get into the routine of achieving seven hours a day. This also has the added benefit of decreasing the likelihood of illness.
Prof Barbara Sahakian from the University of Cambridge, one of the study’s authors, said: “Getting a good night’s sleep is important at all stages of life, but particularly as we age. Finding ways to sleep for older people could be crucial to helping them maintain good mental health and wellbeing and avoiding cognitive decline, particularly for patients with psychiatric disorders and dementia.”
The Sleep Foundation also has similar advice for the ideal slumber time, based on age group.
It suggests that older adults should aim for seven-eight. While the Cambridge study says to go for the lower number in that range, as long as you feel well-rested with the amount you currently get, then it’s all good.
The age at which people can legally buy tobacco in England should increase by one year every year, a government-commissioned review has said.
It recommended the legal age of sale should steadily rise from the current age limit of 18 and millions of pounds be invested to stop smoking.
The independent review by Dr Javed Khan made 15 recommended interventions, including an extra £125 million per year invested in smoke-free policies and a further £70 million per year ringfenced for stop smoking services.
The review also said vapes should be promoted as an effective “swap to stop” tool to help people quit smoking and there should be improved prevention in the NHS offering smokers advice and support to quit.
Dr Khan, former chief executive of children’s charity Barnardo’s, said: “Without immediate and sustained action, England will miss the smoke-free target by many years and most likely decades.
“A smoke-free society should be a social norm – but to achieve this, we must do more to stop people taking up smoking, help those who already smoke and support those who are disproportionately impacted by smoking.
“My holistic set of recommendations for government will deliver this, whilst saving lives, saving money and addressing the health disparities associated with smoking.
“My proposals are not just a plan for this government, but successive governments too. To truly achieve a smoke-free society in our great country, we need to commit to making smoking obsolete, once and for all.”
Dr Khan also called for a “tobacco licence” for retailers to limit the availability of tobacco across the country, a rethink of the way cigarette sticks and packets look to reduce their appeal, and a mass media campaign to encourage smokers to quit.
Almost six million people in England smoke, and tobacco remains the single biggest cause of preventable illness and death, the Department of Health said.
People with monkeypox symptoms have been advised not to have sex by the health authorities.
The UK Health Security Agency (UKHSA) issued this new advice after 71 new cases of the virus were confirmed in England on Monday.
Advertisement
This brings the total to 179 reported cases since May 7, most of which are in England. Four have been in Scotland, two in Northern Ireland and one in Wales.
The monkeypox outbreak has taken the public by surprise over the last month because the virus is usually confined to Central and West Africa, but health experts have been clear that this will not develop into a new pandemic.
Advertisement
Here’s how the authorities believe we can prevent transmission.
Is this virus sexually transmitted?
Advertisement
No – the virus mainly spreads through any close physical contact but can also live on bedsheets or towels.
It also does not spread that easily and there is currently no available evidence that the virus spreads through sexual fluids.
So, why is this the new advice?
As sex encompasses close physical contact avoiding sex would reduce the risk of passing the virus on, according to the health experts.
Advertisement
Anyone who suspects they have the virus should try to cover lesions with clothes, wear a face mask and avoid public transport where possible while they are still potentially infectious.
People only stop being infectious once their lesions have healed and their scabs have dried up – usually in one to two weeks – and so should avoid contact with others until this point.
But, according to the new guidance, people should still use condoms for at least eight weeks after the infection.
The general public have also been advised to keep an eye out for any new rashes or lesions on their bodies.
How do you know if you have monkeypox?
These are the symptoms:
Fever
Headache
Muscle aches
Backache
Swollen lymph nodes
Chills
Exhaustion
Weakness
Rash
UK Health Security Agency via PA Media
UKHSA’s image of monkeypox lesions
The rash can start on the face before moving to the body. It gradually transforms, and can form sores comparable to chickenpox or syphilis before scabbing. The scab falls off but can leave a scar.
The incubation period (the time before symptoms appear) is usually from six to 13 days but can range from five to 21 days.
Why have gay or bisexual men been particularly warned?
Advertisement
The UKHSA report that the majority of cases so far have been among men who have sex with men.
However, it’s important to note that this is likely due to where the virus allegedly first started to spread – at two European raves – and not because this group are at higher risk of catching it.
Anyone is at risk of catching the virus regardless of sexual orientation.
But, she added: “We are concerned that individuals may acquire this infection through high-risk exposure if they don’t have the information they need to protect themselves.”
The UKHSA also said the risk “remains low”, but urges anyone with unusual rashes or lesions to contact NHS 111 or their local sexual health service.
Healthcare workers who are pregnant and people with severely weakened immune systems should not care for suspects or confirmed monkeypox cases.
Those working with confirmed cases need to wear personal protective equipment, including respirators, aprons, eye protection and gloves.
Those at the highest risk have also been asked to isolate for up to 21 days.
Advertisement
Health protection teams are tracing the contacts of positive cases and UK health officials have purchased 20,000 doses of a smallpox vaccine called Imvanex.
This vaccine is said to be relatively effective at reducing severe infection and the rate of transmission – it will be offered to those close contacts of the people who are diagnosed with the virus.
The advice to abstain from sex has not gone down well
Covid affects the heart, lungs and kidneys, according to two new studies, and the impacts could last long after the initial infection has passed.
The first study was carried out in 10 intensive care units across Scotland and examined 121 critically ill patients who were receiving treatment on ventilators due to the impact of coronavirus on their system.
Advertisement
One in three of the patients in the study showed evidence of abnormalities in the right side of the heart – the area that pumps blood to the lungs, researchers found.
Nearly half (47%) of ventilated patients in the study died because of Covid-19, a figure comparable to national and international death rates.
Advertisement
“A combination of factors create the perfect storm for Covid-19 to damage the right side of your heart, which ultimately can cause death,” Dr Philip McCall, lead author of the study and consultant in Cardiothoracic Anaesthesia and Intensive Care at NHS Golden Jubilee, said.
Experts at the NHS Golden Jubilee University National Hospital in Clydebank, West Dunbartonshire, said that the findings could play a vital role in not only saving the lives of Covid-19 patients, but for the care of potentially fatal heart and lung issues generally, as well as helping prepare for any possible future pandemic.
Advertisement
Dr Ben Shelley, chief investigator of the study and consultant in Anaesthesia and Intensive Care at the NHS Golden Jubilee, said: “The study has revealed that there is no doubt Covid-19 affects the heart and has a major impact on outcomes for the patient.
“However, now that we know this actually happens, and have a better understanding of how it affects people, we can plan for the future and put in place new care plans and treatments to help combat this.”
In another study published in the journal Nature Medicine, researchers analysed the outcomes of 159 people hospitalised with Covid between May 2020 and March 2021.
“Our study provides objective evidence of abnormalities at one to two months post-Covid and these findings tie in with persisting symptoms at that time and the likelihood of ongoing health needs one year later,” Prof Colin Berry, of the University of Glasgow, which led the CISCO-19 (Cardiac imaging in Sars coronavirus disease-19) study said.
Advertisement
People who had been hospitalised with Covid showed several abnormalities, including in results from imaging of the heart, lungs and kidneys, the study found.
One in eight of those who were hospitalised for Covid were most likely to have myocarditis, or heart inflammation, experts said. Healthcare workers with acute kidney injury was more likely to have myocarditis as well as those with more severe disease requiring invasive ventilation.
Additionally, people who have been hospitalised with Covid were more likely to need outpatient secondary care or be referred for long Covid, with death and re-hospitalisations also much higher in this group.
Although both studies focussed on patients who experienced severe Covid infection, the results have helped scientists learn about the wide ranging impacts of the virus. Researchers say the findings also serve as a reminder for the general population to stay vigilant about Covid.
Prof Berry added: “Even fit, healthy individuals can suffer severe Covid-19 illness and to avoid this, members of the public should take up the offer of vaccination.”
Covid concerns may have subsided and though they’re far from gone, now another virus, Monkeypox, has been making headlines.
Here’s what you need to know.
Advertisement
What is Monkeypox?
Monkeypox is a rare viral infection that typically does not spread easily between humans. It’s comparable to smallpox but milder, less infectious, and less deadly.
Advertisement
Most people recover within a week and the virus disappears on its own, prompting no long-term health effects. However, a more severe illness can occur in a few people.
The virus usually spreads through close contact with an infected person, although there’s a low risk of transmission among humans.
Advertisement
The symptoms include:
Fever
Headache
Muscle aches
Backache
Swollen lymph nodes
Chills
Exhaustion.
A rash can start too, usually on the face at first before moving to other parts of the body including the genitals. This rash then goes through different changes and can transform to look like chickenpox or syphilis before scabbing. The scabs then fall off, although it can leave a scar behind.
People without symptoms are not considered infectious.
Advertisement
How many cases have there been?
Three cases in London and another in north east of England have just been detected by the UK Health Security Agency (UKHSA), bringing the total up to seven confirmed cases all diagnosed between May 6 and 15.
By May 19, a further two cases had been confirmed by the UKHSA, one in London and another elsewhere in the south east of England.
Those needing urgent care were treated in specialist disease units in hospital, although they were all found to have the West African strain, which is much milder compared to the Central African.
So, why are people concerned?
These four new cases do not have known connections with the previous cases announced earlier in May, although investigations are underway to understand the links between them.
All four individuals were infected in London. They also all self-identify as gay, bisexual or other men who have sex with men.
There’s currently no link to travel abroad to places where monkeypox is currently endemic, meaning the medical community is still uncertain where the individuals picked up the virus.
Chief medical adviser for UKHSA, Dr Susan Hopkins, said that this is “rare and unusual”, and has prompted the health agency to look into monkeypox transmission in the community.
“We are particularly urging men who are gay and bisexual to be aware of any unusual rashes or lesions and to contact a sexual health service without delay.
Advertisement
“We are contacting any potential close contacts of the cases to provide health information and advice,” she added.
The UKHSA’s director of clinical and emerging infections Dr Colin Brown also noted: “While investigations remain ongoing to determine the source of infection, it is important to emphasise it does not spread easily between people and requires close personal contact with an infected symptomatic person.
“The overall risk to the general public remains very low.”
The World Health Organisation (WHO) is now looking into how the virus is circulating and the risk it poses to both endemic and non-endemic country.
They also predicted that case numbers and the number of countries monkeypox is in will rise.
. @WHO is working with member states & partners to better understand #monkeypox circulation in endemic & non-endemic countries. We expect # cases/countries reporting to increase.
Monkeypox is a priority pathogen & requires investment in studies for transmission, severity, R&D… pic.twitter.com/aoxpQY6nTj
The infection is usually picked up from infected animals in rainforests. Minor outbreaks usually occur in West and Central Africa, but transmission is low because it can only happen through direct contact with lesions or respiratory sections.
Infectious disease epidemiologist Mateo Prochazka explained on Twitter just why the new findings were so surprising.
He wrote: “Close contact between two people (such as during sex) could also facilitate transmission – but this has never been described before.”
He continued: “What is even more bizarre is finding cases that appear to have acquired the infection via sexual contact. This is a novel route of transmission that will have implications for outbreak response and control.”
Advertisement
He also pointed out that work is ongoing, especially when it comes to protecting health workers, a sexual health service response and preventing an increase in stigma and inequalities.
Yesterday, @UKHSA reported four cases of monkeypox (MPX) in gay and bisexual men in England, making a total of 7 cases nationally.
The vast majority of respiratory viruses that spread within our population ebb and flow with the seasons.
Influenza spikes in the winter months, as do infections caused by respiratory syncytial virus (RSV), adenoviruses and other coronaviruses. Earlier this year, Rochelle Walensky, director of the US Centers for Disease Control and Prevention, said she expects Covid to also become a seasonal illness – but whether or not that will come to be remains to be seen.
Advertisement
Most scientists agree that Covid isn’t going anywhere, and that we’ll be living with SARS-CoV-2 for decades, if not forever. Though we tend to see the biggest waves in the winter and early spring, Covid isn’t seasonal yet. It doesn’t retreat in the spring-to-summer off-season – it is smoldering throughout the year.
“Covid is steadily burning through the population as we speak. But it is also able to piggy back on top of our ebbs and flows of the typical cold and flu season, so it’s a double whammy,” Mark Cameron, an infectious disease researcher at Case Western Reserve, tells HuffPost.
Advertisement
Will Covid ever become a seasonal illness?
Andrew Noymer, an epidemiologist and demographer who studies infectious diseases at University of California, Irvine, expects Covid to become winter-dominant, like the flu, in the long run. SARS-CoV-2 is already somewhat seasonal and predictable in nature.
Advertisement
“In the United States, all of the largest spikes have been in the winter, so it is kind of seasonal in that respect,” Noymer says.
But, even between those peaks, the virus spreads at pretty significant levels. It hasn’t totally settled into a seasonality. Many epidemiologists thought Covid would have already fallen into much more of a seasonal pattern by now – but it hasn’t.
“A seasonal infectious disease is something that pops up predictably at the start of the cold and flu season and persists throughout that period of time,” Cameron says.
Keep in mind, this is only our third 12-month period with Covid. The illness is still relatively new. Even though over half of the US population and seven in 10 people in the UK have likely already had Covid, others have not and remain susceptible. We’re all antsy for the virus to become predictable, but the virus is still just getting started, Noymer says. He suspects that one day – maybe 10, 15 years from now – we’ll be looking at a very seasonal phenomenon.
Advertisement
Marija Babic / EyeEm via Getty Images
There’s a chance Covid may not become seasonal for years to come.
Is there a chance Covid may never sync up with the flu and cold season and become a winter-dominant illness? Of course, Noymer says. “I can’t absolutely rule out that it never will – that it will be the one exception that disproves the rule.”
The fact that, one, people can get Covid multiple times, and two, that even vaccinated people can catch and spread Covid, makes the epidemiology of this respiratory infection chaotic. Population-level immunity influences when waves occur. After people recover from Covid, they are typically protected from infection for a few months. As time passes, those recently recovered people can become susceptible again. And, on a greater scale, a population can become susceptible to a wave again.
This isn’t an exact science – people get infected and recover at different times. Their immunity wanes at different speeds. “There’s a lot of wheels turning and it’s very hard to predict,” Noymer says.
Here’s what causes respiratory viruses to become seasonal
It’s not entirely clear why respiratory viruses tend to get more active in the wintertime – but they do. Flu activity surges in the winter as do the common cold coronaviruses. Even measles was winter-dominant when it circulated at higher levels in the US, according to Noymer.
“We see this with respiratory virus after respiratory virus after respiratory virus,” Noymer says.
There are a few hypotheses as to why this happens. The first theory is atmospheric conditions – viruses, including influenza, tend to spread more easily when there’s less humidity. Viruses do better in drier conditions.
Another contributing factor is our behaviour. In winter months, when it’s cold outside, we gather indoors together and create plenty of opportunities for viruses to spread from person to person.
Incidentally, this is also believed to be why the US South experiences summer spikes. Contrary to those in the northeast, people living in southern states head indoors during the summer months when the temperature soars and humidity becomes wet and sticky. Schools are thought to contribute to the seasonal spread of respiratory viruses like flu and RSV, Noymer adds.
The behaviour of the virus plays a role, too. The flu, for example, tends to shoot through the population then burn itself out by “mutating to its demise,” Cameron said. Covid, on the other hand, is evolving to become more fit and more transmissible – it’s not acting like a typical respiratory virus that infects people and goes away before bursting back into the population in a different form months later.
Advertisement
If we look to other circulating coronaviruses that cause the common cold, we can reasonably expect Covid to eventually become endemic and more seasonal in nature, according to Cameron. But we don’t know when those coronaviruses settled in their seasonality. How long that will take with Covid is a mystery. This is wide-open territory that has yet to be studied.
“How can we understand how long Covid will take to become just another garden-variety coronavirus that is circulating and causing sporadic disease?” Cameron said. “It certainly isn’t now.”
Experts are still learning about Covid-19. The information in this story is what was known or available at the time of publication, but guidance could change as scientists discover more about the virus.To keep up to date with health advice and cases in your area, visit gov.uk/coronavirus and nhs.uk.
You’re reading Move, the nudge we need to get active, however makes us happiest and healthiest.
For many fitness lovers, leg day is often the least favourite of the week. But that’s often because of the misconception that you have to push your body to the point of struggling to walk the next day.
Advertisement
Instead, why not try a short but effective lower body workout?
David Wiener, training and nutrition specialist at Freeletics, has shared a five-minute circuit with HuffPost UK that can be added into your next gym session or practiced during spare moments of the day.
Advertisement
“Lower body exercises are beneficial and vital for making daily tasks, such as walking, easier on us. Performing these exercises not only improves your stability, but it is a chain reaction on the rest of your body for helping improve your strength and posture,” he says.
“Ultimately, improving your lower body workout routine will give you lean muscle and achieve a stronger and more toned lower body, including the calves, thighs, hamstring and glutes.”
Advertisement
Try the “no glutes, no glory” workout today and you’ll never* be tempted to skip leg day again.
(*Well, until next week at least.)
1. Squat Jumps
Freeletics
This exercise is great because it’s an all over body work out, but especially good for the lower body. It can help build your muscle and enhance strength, as well as boost your cardiovascular fitness, tone your lower body, strengthen bones, boost your circulation and burn many calories.
Advertisement
To do one: Start standing with your feet about shoulder-width apart. Point your toes slightly outwards. Always keep your back straight. Always keep hands off your body.
Lower down until your hips are below knees. Jump up so both feet leave ground and then return to the starting position before repeating.
2. Lunges
Freeletics
Freeletics
Lunges are a great exercise to increase the muscle mass in your lower body whilst building up your strength and toning. Not only this, they also help to improve your posture, balance and range of motion. Whilst a lot of exercises put strain on your spine, lunges help give your spine a chance to relax whilst working many of the larger muscles in the lower body.
To do one: Start standing upright, with your hands on your hips. Always keep your shoulders above the hips. Step forward with one foot Keep your front foot flat on the ground. Bend your back knee so it touches the ground below your hip Alternate lunging leg for the desired number of reps.
3. Squats
Freeletics
Much like a jumping squat, a normal squat has similar benefits but not as much cardio. Whilst this exercise will of course not burn as many calories as a jumping squat, it is still a great exercise to put your quadricep group of muscles to work. There’s a misconception that squats put too much pressure and strain on your knees, but squats will actually strengthen your knees and make them less prone to injury as you get older.
To do one: Start standing with your feet about shoulder-width apart. Point your toes slightly outward. Always keep your back straight. Always keep hands off the body. Always keep weight toward your heels. Lower down until your hips sit below your knees and rise back up to the starting position
Advertisement
4. Split Lunges
Freeletics
Much like the normal lunge, split lunges are a great way to work your quads, glutes, hips and hamstrings. As they are a unilateral exercise (meaning they only train one side of your body at a time), they are proven to increase your balance and posture too. Not only this, your hip flexor muscles are most commonly tight, but performing split lunges will help you improve the mobility of these muscles.
To do one: Start standing upright. Always keep your shoulders above the hips. Step forward with one foot. Keep your front foot flat on the ground. Bend your back knee to touch the ground below hip. Jump up to switch sides. Make sure your feet leave ground at same time.
Rest.
5. Table Twists
Freeletics
To enhance the flexibility of your lower body and spine, table twists are simple to perform and will stretch out all the major muscle groups in your body, helping to boost flexibility and enhance range of motion.
To do one: Start with your hands below your shoulders, heels below the knees, and hips on ground. Push up until your hips are in line with your shoulders and knees. Reach one hand up and behind you. Return to the starting position. Alternative sides Always keep your arms straight.
Rest and repeat.
Move celebrates exercise in all its forms, with accessible features encouraging you to add movement into your day – because it’s not just good for the body, but the mind, too. We get it: workouts can be a bit of a slog, but there are ways you can move more without dreading it. Whether you love hikes, bike rides, YouTube workouts or hula hoop routines, exercise should be something to enjoy.
On January 22, 1973, the US Supreme Court affirmed in a 7-2 decision the legality of women’s right to have an abortion under the 14th Amendment.
Today, about one in four pregnancy-capable people in the US have had an abortion, and the risk of complications from an in-clinic procedure is extremely low. But before it was guaranteed as a constitutional right, seeking an abortion was a harrowing, potentially life-threatening endeavour.
Advertisement
While some women saved up the cash and sometimes travelled hundreds of miles to find qualified medical providers willing to risk their livelihood by operating on patients, others settled for providers lacking the qualifications and skills to perform induced abortions. And even more desperate people attempted their own abortions.
The outcome of these back-alley procedures or at-home coat-hanger abortions was often devastating, leading to maternal death or lifelong injury. (Complications from unsafe abortions include infection, incomplete abortions, haemorrhaging, uterine perforation and damage to the genital tract or internal organs, according to the World Health Organisation.)
Advertisement
Because these stories were so traumatic – and because the stigma surrounding abortion was even greater in those pre-Roe v. Wade years – many women remained silent about their experiences.
Now, as the US Supreme Court seems poised to overturn the Roe v. Wade decision, it’s worth revisiting their stories to understand what abortion was like in the decades before it was legalised.
Advertisement
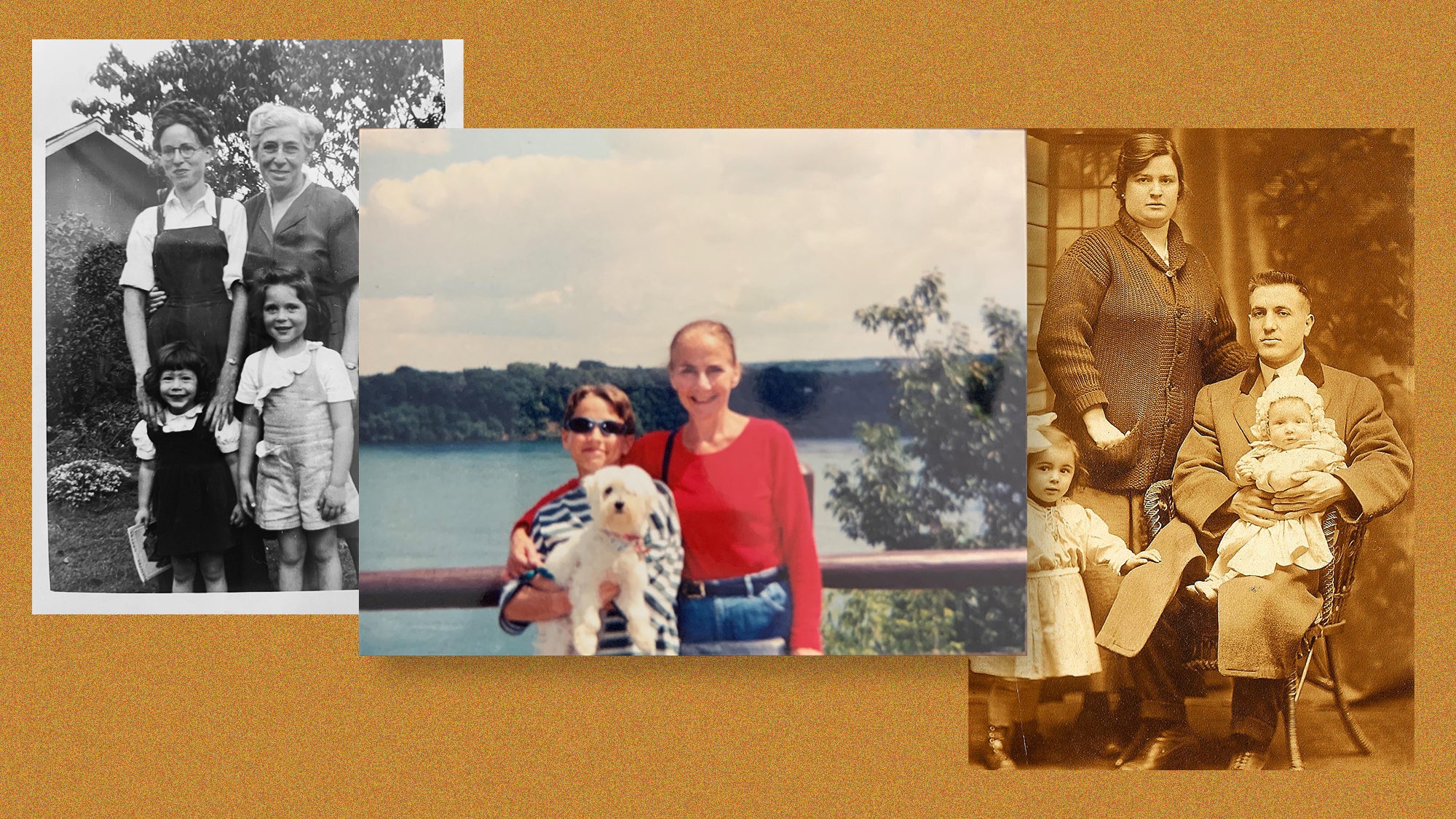
HuffPost US recently spoke to eight people who shared experiences of relatives – great-grandmas, grandmas, mothers and aunts – who sought abortions in pre-Roe v. Wade America. Many were already mothers, struggling to conceptualise raising one more child in poverty or, in some cases, with an abusive spouse.
In one story that differs from the rest, a reader shares how her great-grandma, the wife of a well-to-do dentist, was able to obtain a safe abortion in a doctor’s office with little fuss; the story illustrates how white, middle-class and upper-class women have always had an easier time accessing safer abortion options. (As many have noted, women of colour will be disproportionately affected if Roe v. Wade is overturned.)
Below, read all eight stories, which have been edited lightly for clarity, style and length.
“My maternal grandparents married in 1934.By the time my mother was born, it was clear my grandpa was a monster. Violent and cruel, he beat my grandma with a metal lunchbox. When mom was just a few months old, he threw her against a wall. My grandmother fled.
Advertisement
She discovered she was pregnant again. To induce an abortion, she drank a bottle of Lysol. You can Google ‘Lysol abortion’ and see ads from that time that suggested a woman could use Lysol to ‘correct your mistake.’ The ads are quite chilling, their meaning vague and without instructions.
Was reading the Dec 2019 edition of The Atlantic. Learned that Lysol was marketed as a “feminine hygiene” product and often used by women seeking abortions when they were illegal in the US.
It took my grandma 29 hours to die in her parent’s home; they were helpless to end the agony. Living in a logging village in winter, there was no hospital or way to travel to the city.
My mother always felt responsible for her mother’s so-called ‘suicide,’ as children do. Doing genealogy research, I uncovered the full story when my mother was in her late 60s, but her life was already written and the truth brought no comfort. I sometimes think I should never have done the research. There are four generations impacted by this one attempted abortion. We can never really know how lives would be different if she had lived. But I do know my mother’s life was forged by that event, she was an orphan, hidden from her father, never knowing why she’d been abandoned.” – Chuck M., 62, from Washington state
“My mother was a 16-year-old in 1970when she became pregnant as a result of sexual assault. She was living with my grandparents in Southern California, and abortion was not legal at that time. My grandparents were not in a position to get over the border into Mexico to have the procedure done, and they didn’t have access to a safe place to have the procedure done, either. Rather than risking my mother in a back-alley abortion, my grandmother assisted my mother in inducing a miscarriage. My grandmother had my mother sit in steaming hot baths for hours. My mother ingested medications that were considered dangerous to a fetus. They did everything short of physically harming my mother, though my mother did tell me that she was so desperate to end the pregnancy that she considered throwing herself off a high platform or down the stairs.
They managed to successfully induce a miscarriage, and my mother was taken to the local hospital to deal with the effects of the miscarriage and for a dilation and curettage. That worked, but her young body and mental health were not OK. Though my grandmother’s and mother’s intentions were to do something safer than a back-alley abortion, my mother was still at risk of potential harm from the various medications she took. And the foetus would also have been at risk for birth defects and other issues if the medications had not succeeded in a successful miscarriage. It was still dangerous.
My mother told me once that Roe was the single most important law that passed in her lifetime. That she was relieved that other women and people with a uterus would not have to suffer the same circumstances she did. If she were alive today, she would be absolutely shattered.” – Sara from New York
“My aunt Judith was just 17 in 1964 when she became pregnant after being raped on a study date at a so-called friend’s house. She was horrified to find out she was pregnant; she was on her way to college in the fall, and a baby wasn’t in her plans yet. Her doctor suggested a girls home out of town where she could stay until the baby was born and then give it up for adoption; it was her only choice since abortion was illegal.
Judith had tried all the old wives’ tales, jumping backward a dozen times at dusk and even drinking a tea that made her deathly ill just to lose the pregnancy naturally, but nothing worked. A friend of hers, Arbie, who was two years older, had been in Judith’s shoes and had taken care of her ‘dilemma’ herself.
In that summer of 1964, Judith chose to use a metal coat hanger, thinking it would be over quickly and no one would ever know. Her end result was far more than she had ever anticipated, with excessive bleeding and infection that led to a partial hysterectomy and the inability to ever carry a child. She spent nearly a month in the hospital. Her mother found out and never looked at her the same, although she did keep [Judith’s abortion attempt] from Judith’s father, knowing he would have kicked her out and pulled her college tuition. The family was hush-hush about everything, given the era everything took place.
Judith went on to graduate college top of her class to become the first female doctor of psychology in the family. From the outside looking in, her life was perfect: the house, her own office, nice car, all the material things one could ever hope to have, but she had developed a serious drinking problem and her life behind closed doors was, as she once said, ‘exactly what you’d think hell on earth would be.’
Advertisement
I was born in ’72, her only niece at the time, and she doted over me constantly every chance she had. I never suspected anything was ever wrong, although I did always wonder why Auntie Judy had such sad eyes; it wasn’t until puberty hit for me that she warned me of the dangers of having ‘that time’ and told me her story. She explained there were no real options in ’64 but said that because of Roe v. Wade in ’73, I would have more options than she had ever had.
Her desire to be able to carry a child, to be the mother she had always dreamed of, haunted her every waking hour and her dreams, and she was never able to get away from it. In 1984, just a week shy of her 37th birthday, my Auntie Judy hung herself in her attic; the pain and anguish had finally won the battle. Her note was a short novel, telling her story. I was only 12 and was told I wasn’t old enough to read it or understand it, but I didn’t listen. I sneaked and read it, and now I can remember every word, and her pain, longing and anger still haunt me to this very day.” – AJ, 50, from Louisiana
Jared Milrad/Canva
“Like most kids raised by a single mother, I’ve always thought of my mom, Jan, as courageous, resilient and strong. Growing up, she commuted nearly two hours each day ― every day ― to work a low-paying job as a secretary so that my brother and I could have a better future. Despite all that she went through, my mom never gave up and ensured that my brother and I could get the best education and have more opportunities than she did.
But it wasn’t until I was in my 20s that I realised how truly incredible my mom is. One day, my mom shared that she was around my age when she had two abortions. This was 1968-69, when abortion was still illegal in the U.S. and my mom was 26 or 27 years old.
My mom told me that she had her first abortion during this time while dating a much older man. The pregnancy was very unexpected, and because my mom was struggling to make ends meet and didn’t have much support at all, she made the wrenching decision to abort the pregnancy. Because abortion was illegal in the States, the man found a doctor for her in Puerto Rico and agreed to pay for the procedure, so my mom went with my grandma to have it done. They traveled to San Juan and then traveled a bit outside of the city. My mom expected the procedure to be done with anaesthesia, but – horrifyingly – it wasn’t.
‘The abortion was done by a butcher and my mother heard me screaming,’ my mom recalled. ‘I didn’t know that they weren’t going to give me anaesthesia. It lasted for only 20 or 30 minutes, but it seemed like a lifetime. When we got back to the hotel in San Juan, I was in such pain. Then, when I was back in New York City in A&P Grocery a few days later, I noticed that I was bleeding ― haemorrhaging.’
My grandma immediately called a gynaecologist and arranged to have my mom treated in the ER at Lenox Hill Hospital, where they didn’t tell the doctors that the bleeding was caused by an abortion out of fear because the procedure was still illegal. My mom was lucky to survive.” – Jared Milrad, 38
“Today, the majority of women who seek a legal abortion are already mothers. Let me share a pre-Roe horror story about my Italian, Catholic grandmother Mary, whom I never had the blessing to know.
Apparently, on her deathbed in 1943, Mary asked her sister-in-law Florence, who was childless, to take care of her only daughter, but the shameful secret had to be kept. My mom was forbidden to ask questions about her mother or her death. She learned the truth when she was in her 50s from me after years of research.
I was in my 20s when I first began to put together the pieces of a story that just didn’t make sense: a 34-year-old mother of three young children who is hemorrhaging but refuses to go to the hospital. Even the death certificate corroborates the secret. Cause of death: carcinoma of the cervix. But cervical cancer does not generally cause women to bleed to death.
Advertisement
Then, one day in the mid-’70s, we were talking about the Roe decision, and Florence, the woman I knew as my grandmother, let it slip that she had to lend $250 (an enormity in 1943) to one of her brothers because someone needed an abortion. I was stunned; I finally connected the dots. In a typically large Italian Catholic family, Florence had many sisters but only two brothers. One of them, it turns out, was my biological grandfather.
Grandma Mary already had three children she loved: two boys and the middle child, my mom Nancy. With an unemployed husband, a fourth child would plunge the family into poverty.
So the decision was not made lightly, but something went horribly wrong. Mary was just 34 years old and was more afraid of the law (and the judgment of the Catholic church) than she was of dying and leaving her children motherless.” – Lori Bores from New York
“Great-Grandma Selma Rosenthal (born 1878) was a career woman.Graduating from college in 1901, she was homely and smart, two things that did not make her particularly attractive to suitors of the era. Knowing this, she focused on having a successful career. She was by all accounts very funny, with a wonderful voice and an active circle of friends. She had no expectation that marriage or family were in the cards for her, and she had made peace with that idea.
That all changed when she met Sidney Rauh, a dentist from Cincinnati from a well-off family. It was the 1910s, and she was well into her 30s. Sidney was equally unattractive and clever, and a confirmed bachelor. He had no interest in marrying a girl for her looks but wanted to find someone he could love for her mind. When they met, it was love at first sight, and given their advanced ages, they decided to marry as soon as possible.
Selma quickly became pregnant, only to miscarry the first Christmas they spent together as a married couple. Two daughters quickly followed in 1916 and 1919, but Selma was terribly sick with her second pregnancy and she barely survived childbirth. Her doctor told her, in no uncertain terms, that if she was to get pregnant again and attempt to see it to term, she would die. She promised she would be careful.
A few years later, when she realised she was pregnant, she went to her doctor. The doctor advised her that she had to have an abortion. Sometime later, the doctor performed an abortion in his office, no fuss, no muss. But Selma was a well-off wife of a successful dentist with status in the community. It never occurred to her that what she was doing was illegal or in any way wrong. It was a decision between her, her doctor, and Sidney, and she did what was best for her family and health.
Selma died in 1948 at the age of 62 of a heart attack, having spent time not just with her daughters, but also with her granddaughters, who were five and three at the time of her death.
Great-Grandma was a suffragette and strived for women’s rights. Women’s rights and bodily autonomy were key issues in my family, but I suspect the story would not have been noteworthy had it not been for the fact that abortion became the issue it was later on. My mother and grandmother shared with me how hard things like birth control had been to get in their era, and my mother shared with me the fact that she got a (legal) abortion for family planning reasons. For us, it was just part of normal conversation.” – Kate, 50, from New York
Stephanie Voltolin/Canva
“I was born in the 1960s and grew up in a very conservative Catholic family. Nonetheless, my traditional housewife mother was ardently pro-choice. She even took one of my friends to get an abortion in the 1980s because my friend couldn’t tell her family she was pregnant.
Advertisement
Shortly after my paternal grandmother died, when I was a college freshman, my mother frankly told me during a conversation about choice, ‘Your grandmother had a back-alley abortion and almost bled to death.’
My grandmother found herself – in the early 1940s before birth control or abortion were legal – pregnant and divorced from her second husband, who turned out to be horribly abusive. She decided to leave before he began abusing her three children from her first marriage. Like most women of her day, she had no college education or career to support herself and her children. And, like most women who get abortions, she could barely support the children she had. She ended up having to go live with her parents, who were Italian immigrants.
Faced with being twice divorced and pregnant, my grandmother sought an abortion. Because they were illegal, she had to trust a back-alley ‘doctor,’ who punctured her uterus in the process. She left the procedure, collapsed in the street from the blood loss, and had to be taken to the hospital. An emergency hysterectomy saved her life.
She was an amazing mother and grandmother, and although she died almost 40 years ago, I still become emotional when I think about what a loss I would have suffered had she died from that botched abortion.
The rest of the family never knew. I am telling her story now in the same way that we disclosed our sexual trauma during the Me Too movement to educate others. Legal and safe abortion is critical to women’s reproductive rights as American citizens, and we cannot allow them to expire.” – Stephanie Voltolin
“My great-grandmother died from a botched, illegal abortion in the mid-1930s in Chicago, leaving my grandmother (2 years old) and her sister (4 years old) without a mother. When my great-grandfather remarried, his new wife already had kids of her own and didn’t want to take care of two more. My grandmother and her sister were thrown out of the house and bounced around to different aunts and uncles.
For much of my grandmother’s life, she was told that her mother died of a pregnancy complication due to an ectopic pregnancy. Later, when my grandma was a teenager, her aunt told her the truth: that her mother had died from a botched, illegal abortion.
My grandmother shared her story with me in 2012 when I was 25. We were having an early lunch. I remember she asked me if I wanted a glass of wine, which was odd for her in the middle of the day. We were talking about something else entirely and she said, ‘my mother died of a botched, illegal abortion,’ almost out of the blue, and her story just unfurled from there.
I honestly didn’t think too much about what my grandmother shared. I didn’t think her story was shocking or novel, maybe because abortion had been legal in all 50 states for my whole life. I assumed everyone else in our family knew, so I didn’t think to say anything.
A couple years later, I was catching up with my parents and one of them said, ‘Did you know Great-Grandma Sally died from a botched illegal abortion?’ That’s when I realised my grandma was nervous when she shared her mother’s cause of death with me. She was holding on to this family history and likely carrying with her the shame and stigma or the ‘don’t talk about it’ attitude of her family. It was an ‘aha’ moment for me – a real understanding that likely everyone has a family abortion story, whether they know it or not.
Advertisement
Now our family has a deep understanding that when abortion is legal, abortion is safe. And we know in the decades before Roe v. Wade was decided, people like my great-grandmother were desperate to receive the care they needed.” – Amy Handler, 35, from Oregon