Families across the UK have been urged to stay vigilant about Strep A symptoms this week, following a series of tragic deaths in children.
A total of 15 children have now died in the UK from Strep A since September, according to the latest figures. This includes 13 children under the age 15 in England and two others in Northern Ireland and Wales, according to data from the UK Health Security Agency (UKHSA).
Advertisement
Streptococcus A (Strep A – also known as Group A Strep or GAS) are a group of bacteria that can cause a wide variety of skin, soft tissue and respiratory tract infections. These include strep throat and impetigo, but the most common illness caused by Strep A is scarlet fever, which is highly infections and has been spreading across the country.
But why are infections so awful this year? And what – if anything – can parents do about it?
Why is Strep A spreading?
Less mixing due to Covid could be part of the reason why hundreds of children are being diagnosed with Strep A-related illnesses this year. When social measures were put in place, the spread of Strep A was contained. Now, children who did not catch Strep A in 2020 or 2021 are being infected.
“It strikes me that as we are seeing with flu at the moment, lack of mixing in kids may have caused a drop in population-wide immunity that could increase transmission, particularly in school age children,” microbiologist Dr Simon Clarke, from the University of Reading, told Sky news.
What are the symptoms?
The best way to protect your kids is to know the symptoms and seek treatment quickly. It’s important to remember that Strep A causes a mild illness in the majority of children that can be easily treated with antibiotics. Symptoms include:
Advertisement
- red and white patches in the throat
- trouble swallowing
- a headache
- lower stomach pain
- general discomfort, uneasiness, or ill feeling
- loss of appetite
- nausea
- rash
“On darker skin, the rash can be more difficult to detect visually but will have a sandpapery feel,” Duncan Reid, pharmacist at Pharmacy2U told HuffPost UK.
Additionally, the British Islamic Medical Association explained that “the rash is more obvious in the groin/armpit area. Sometimes the flushed cheeks appear as ‘sunburned’ on darker skin with whiteness near the mouth”.
“In children with darker skin tones, the rash could be harder to spot as it may not appear red, but will be darker than normal skin,“ Dr Mabs Chowdhury, president of the British Association of Dermatologists added.
“The rash in all pigment types can have a sandpapery feel. The tongue can appear redder than normal with prominent white spots (sometimes called ‘strawberry tongue’).”
Advertisement
Where are the infections in the country?
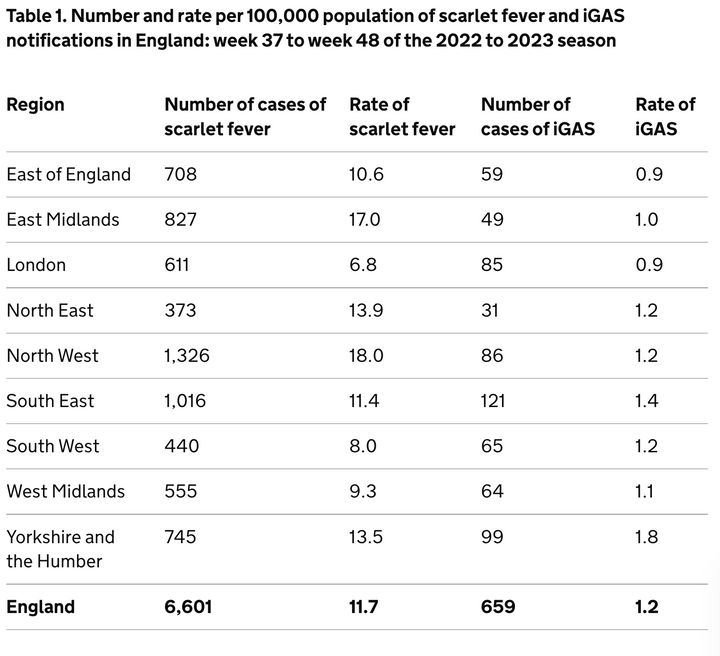
The latest available data shows that in England, there were 1,062 scarlet fever infection notifications received in week 48 (the week commencing November 28).
Currently, there are large concentrations of Strep A and associated scarlet fever cases in multiple parts of the UK, with the North West particularly impacted. The below data also shows incidences of invasive group A streptococcal infection (iGAS) – a rare but serious complication of Strep A, which can be life-threatening.
How do parents feel?
Plenty of parents are beside themselves with worry right now as strep A continues to dominate the news. On social media and in private Whatsapp groups there’s been an outpouring of worry from parents, who are understandably on edge in case they miss the signs of illness that could progress to something far worse.
Advertisement
“I’m personally more worried about this than I was when Covid started,” said 35-year-old Emma Hawes from Wigan.
Hawes, who has a 13-year-old and eight-year-old, told HuffPost UK: “I am extremely anxious at the moment. I had no idea what the symptoms were so I’ve obviously been reading as much as I can.”
Diana Wilkinson, 45, has two children of primary school age. She told HuffPost UK: “I’m genuinely so worried about it. Every time I see the news it’s full of warnings of Strep A, and horrifically the number of fatalities is rising.
“Our school has been great at flagging concerns and sending out information about what to look out for, but with several cases already it feels very close to home.”
Is there an antibiotics shortage?
Some pharmacists are warning of a shortage of antibiotics – which hasn’t done much to quell concerns. However, the government has repeatedly denied it.
Advertisement
The National Pharmacy Association explained: “Pharmacies are having to work very hard to obtain stocks of these antibiotics and some lines are temporarily unavailable.
“We have been advised by wholesalers that most lines will be replenished soon, but we cannot say exactly when that will be.”
Leyla Hannabeck, CEO of the Association of Independent Multiple Pharmacies, claimed that authorities going on broadcast rounds saying there is supply is “misleading”.
“I want to reassure the public that pharmacies are doing everything we can to get hold of antibiotics and we are pushing the government to identify where the blockage is,” Hannabeck added.
Health secretary Steve Barclay said there was a “good supply” of penicillin, and that he had been reassured by medical suppliers. However, he said some GPs may experience shortages as stock is moved around to meet demand.
Advertisement
“Now, sometimes, GPs can have particular surges if they’ve got a lot of demand in an area, and that’s quite routine, we can move the stock around our depots,” he told Sky News.
Will schools close?
Currently, the Department for Education (DfE) has not updated its official advice to schools, but it is directing them to guidance from the UK Health Security Agency (UKHSA).
Parents were told to keep their children at home if they suspected that their children had Strep A, in a blog published by Dfe.
Education secretary Gillian Keegan said the department was “working closely” with the UKHSA and “monitoring the situation”, adding that the situation is “worrying”.
One school in Hull temporarily closed for a “deep clean” after several Strep A cases, but at the moment, schools on the whole are not being advised to close.
Advertisement
How do you catch Strep A?
“Some people can have the bacteria present in their body without feeling unwell or showing any symptoms of infections and while they can pass it on, the risk of spread is much greater when a person is unwell. It is still possible to infect others for up to three weeks.”
“Good hand and respiratory hygiene are important to top the spread of Strep A. By teaching your child how to wash their hands properly with soap for at least 20 seconds, using a tissue to catch coughs and sneezes, and keeping away from others when feeling unwell, they will be able to reduce the risk of picking up or spreading infections.”
When should parents contact their GP?
- if you suspect your child has scarlet fever
- your child is getting worse
- your child is feeding or eating much less than normal
- your child has had a dry nappy for 12 hours or more or shows other signs of dehydration
- your baby is under 3 months and has a temperature of 38°C, or is older than 3 months and has a temperature of 39°C or higher
- your baby feels hotter than usual when you touch their back or chest, or feels sweaty
- your child is very tired or irritable
- your child is having difficulty breathing – you may notice grunting noises or their tummy sucking under their ribs
- there are pauses when your child breathes
- your child’s skin, tongue or lips are blue
- your child is floppy and will not wake up or stay awake.