Depression is an extremely common mental illness, affecting 1 in 6 adults in the UK and usually in combination with other mental health conditions like anxiety, stress, and loneliness. It’s still a massively undertreated condition with only 15% of women getting treatment for it and 9% of men. Women are also twice as likely to experience depression than men.
The differences don’t end there, though.
It turns out that the way the two sexes react to and experience the symptoms of depression are different, too.
Advertisement
Depression Between The Sexes
Depression can hit as early in life as adolescence and for girls, this means struggling with body image, guilt, feelings of failure, difficulty concentrating and general sadness. For boys, this manifests as losing interest in their usual activities and to be more downcast and tired in the morning.
As they get older, women are more likely to see their depression manifesting with stress, sadness, and sleep problems while men will experience irritability and anger outbursts.
Why Do The Sexes Experience Depression Differently?
A new study of over 270,000 participants found that prediction methods that take into account gender are more precise in determining an individual’s genetic predisposition to depression than those that do not consider gender.
Advertisement
Until now, depression has been treated without gender being considered but this research has highlighted the importance of gender-based treatments due to both the body’s development of the illness and the widely different ways that it can manifest.
The researchers found 11 sections of DNA associated with depression in women and only a single section in men.
This study also found that depression was linked to metabolic diseases like diabetes and also linked to obesity in women.
Researchers hope that this first-of-its-kind study will help to guide future gender-specific treatment.
Get Help With Depression
If you’re struggling with depression or think you could be, speak to your GP to get the support that you need. Treatments for depression can include talking therapies and medication. Your GP will work with you to identify the best treatment for you. The mental health charity Mind has advice on resources for mental health self-help too.
Thousands of patients who suffer from the worst migraines will be offered a potentially life-changing drug on the NHS in England after it was approved by the health watchdog.
The National Institute for Health and Care Excellence’s (Nice) draft guidance published on Wednesday recommended the drug Rimegepant as an option for preventing migraines in up to 145,000 adults, if previous treatments have failed.
Advertisement
The Migraine Society says attacks usually last between four and 72 hours and symptoms include disturbed vision, sensitivity to light and sound, feeling sick and vomiting.
Nice says more than 5.6 million people in England are thought to have episodic migraines and around 190,000 attacks are experienced every day.
Beta-blockers, antidepressants and epilepsy medicine are used to try to help with the headaches, but can have significant side-effects and can be ineffective, according to Nice.
Injections are also used to try to solve migraines, Nice added.
The draft guidance recommends the pill, made by Pfizer, for adults who have at least four migraine attacks a month but fewer than 15.
Advertisement
Rimegepant is taken as a wafer which dissolves under the tongue.
Final guidance is expected next month if there are no appeals.
Helen Knight, Nice director of medicines evaluation, said: “Each year the lives of millions of people in England are blighted by migraine attacks.
“They can be extremely debilitating and can significantly affect a person’s quality of life.
“In comments received during consultation on the previous draft guidance, patients and carers described migraine as an invisible disability that affects all aspects of life including family, social activities, mental health, finances and education.
“Rimegepant is the first oral treatment for migraine to be recommended by Nice and for many thousands of people it is likely to be a welcome and more convenient addition to existing options for a condition that is often overlooked and undertreated.”
Toby Cousens, head of hospital and internal medicine at Pfizer UK, said: “On top of debilitating physical symptoms, migraine can place significant pressure on the professional and personal lives of those living with it, including being forced to take time off work.
Advertisement
“Today’s decision is a positive step forward to help meet the care needs of eligible patients in England and Wales.
“We are committed to improving the lives of those living with the burden of migraine and will continue to work with Nice and other health bodies in the UK to help further enhance access and care.”
My daughter, Sammie, was three months shy of her second birthday when she was diagnosed with cystic fibrosis (CF). All I knew about CF at the time was that long ago, on my dad’s side of the family, a couple I never met lost two children to a disease.
Our paediatrician gently broke it to us before sharing the “good news” that the average lifespan of a person with CF had reached 31 years. My husband and I sat in stunned silence. I was 31.
Advertisement
Cystic fibrosis is a progressive genetic disease that clogs the airways, pancreas and other organs with a thick, sticky mucus, impeding breathing and digestion as it slowly destroys the lungs. While there’s still no cure for the disease, the newest generation of treatments targets the underlying defect — a dysfunctional protein — to prevent that sticky mucus at a cellular level.
The most powerful of these drugs is called Trikafta, and Sammie, now 26, is lucky to be on it. She still has a life-threatening, chronic illness — but she was offered a lifeline not everyone gets.
Courtesy of Abby Alten Schwartz
Sammie’s 7th birthday party.
Recently, our good fortune was underscored by two experiences in the same week — polar extremes that encapsulate the emotional rollercoaster of life as a CF parent.
Advertisement
On Facebook, I posted messages of love and remembrance to two different friends on their daughters’ birthdays. Though more than a decade has passed since they died from CF, these vivacious young women will be forever frozen at ages 22 and 13.
Days later, I read the results of a recent U.K. study on the long-term clinical prognosis for CF patients taking Kaftrio (sold as Trikafta in the United States). Based on a simulation model, researchers concluded that the triple-combination drug can substantially increase survival for people with CF, and when started between the ages of 12 and 17, could lead to a “near-normal life expectancy” of over 82 years.
I knew this drug was a game-changer, but reading those words in a medical journal felt surreal. I cried, exhaling the breath I hadn’t realized I was still holding.
Courtesy of Abby Alten Schwartz
The author and her husband with Sammie on a trip to NYC after high school graduation in 2015.
Five years ago, my daughter enrolled in the Phase 3 clinical trials for the triple-combo drug. We were thrilled when her CF care centre was selected as one of the research sites and relieved she met the criteria. She’d been too sick for inclusion during Phase 2.
Advertisement
Within hours of taking her first pills, Sammie coughed so violently she had to leave class. Her lungs were expelling mucus — what the CF community now refers to as “the purge.” When she told me what was happening, I felt the first stirrings of hope. I wondered, “Could this really make a difference?”
The pills made a difference. Within a week, her lung function reached levels she hadn’t attained since middle school. Within months, her blood sugars stabilised, and she was able to stop injecting herself with insulin for her CF-related diabetes, a frequent complication of the disease. Most noticeable was the disappearance of her telltale cough.
My daughter still takes dozens of medications to maintain her health, but the burden of treatment has lightened substantially. She no longer needs twice-daily nebuliser treatments and respiratory therapy using a pulsating vest to shake the mucus from her airways (this varies by patient — some still need daily therapy, others only when sick).
In October 2019, the FDA approved the new drug. Three-and-a-half years later, I’m still overcome with gratitude for this miracle of science — the most significant research breakthrough in the history of cystic fibrosis since the discovery of the CF gene in 1989.
Courtesy of Abby Alten Schwartz
The author and her husband with Sammie cheering on the Phillies at Citizens Bank Park in 2019.
Advertisement
Genetically, I am linked to that history. It turns out those distant relatives, my cousins Dr. Milton “Billy” Graub and his wife, Evelyn, were among the group of parents who started the Cystic Fibrosis Foundation in Philadelphia in 1955. Now based in Bethesda, Maryland, the organisation has since expanded into a nationwide network of accredited care centres and a model of venture philanthropy, an innovative approach to funding research that has been widely lauded.
For the first time since her diagnosis, my daughter has a good chance at living a long and healthy life. At the very least, this drug is buying us time until scientists reach the next milestone.
I feel deep appreciation for the countless individuals who gave time, money and effort to support the research and programs that help CF families like mine. I’m also mindful that CF progresses differently in each patient and continues to take lives every day. I’m in awe of the families grieving loved ones who choose to keep fighting to eradicate this disease.
Not every patient can take this drug. For some, side effects like liver problems or extreme depression outweigh the benefits. For others, the high cost of the drug, disparities in insurance coverage, and barriers to access in certain countries mean more lives will be lost while an effective treatment remains just out of reach. And though it targets the gene mutation (F508del) found in 90% of the CF population, the triple-combo doesn’t help all mutations, leaving some patients waiting and hoping they won’t be forgotten.
Courtesy of Abby Alten Schwartz
The author and Sammie flying pre-pandemic. “People with CF have to be cautious about exposure to respiratory viruses — even a cold can develop into a lung infection,” she writes.
Advertisement
Being one of the lucky ones comes with responsibility. I’m profoundly grateful to the scientists who very likely saved my daughter. I also know it could just as easily have been her receiving posthumous birthday wishes. Every age Sammie reaches that my friends’ girls never will is a blessing and a gut-punch. Every major moment — from college graduation and her first full-time job to all the possibilities ahead — sparks happiness tempered by humility.
I shared my thoughts with a friend, referring to my conflicting emotions as a kind of survivor’s guilt. My friend pointed out that I haven’t survived anything. What is the term, then, for feeling simultaneously thankful my child has been granted the gift of a future and loath to celebrate too loudly?
I don’t want to hurt my fellow CF parents who, by random genetic selection, are witnessing a segment of the CF population improve while their loved ones decline. Or worse — are mourning a child who might have been helped had this drug arrived sooner.
I don’t take our good fortune for granted. Though my daughter’s health and prognosis have improved, CF affects her every day, and I’ve seen too many times how quickly the course of this disease can accelerate or take an unexpected turn. I’m also painfully aware of the fragility of our situation. A change in the supply chain, health insurance, or her tolerance of the drug could suddenly revert my daughter to her previous condition — with a chronic cough, compromised lungs and a precarious future.
Courtesy of Taylor Melchior
Sammie graduated from Temple University in August 2020 without a ceremony.
Advertisement
Earlier this month, the triple-combo pill was approved in the U.S. by the FDA for expanded use by children ages 2-5 with the targeted mutations. As with every step forward in fighting this disease, it’s vital that we recognise the systemic problems that keep many individuals who need this drug from accessing it.
Like many specialty drugs, this one comes with a prohibitive price tag — over $300,000 per year. Thankfully, because of its proven effectiveness, most insurance companies have added it to their formularies. But not everyone has insurance. And while the manufacturer helps families like mine with copay assistance, other families were shocked to learn their assistance would be limited this year due to controversial “copay accumulators” some insurance companies started adding to their policies. Many affected by this change were able to get grants from groups like The HealthWell Foundation, solving one problem but highlighting the unpredictable — and inequitable — reality of living with a chronic or life-threatening illness.
The disease itself is only one of the threats families like ours face. Whenever there’s movement to dismantle the Affordable Care Act, it’s not just people with preexisting conditions at risk, but anyone who needs an expensive drug or treatment — or one day will. The ACA prohibits insurance companies from setting annual and lifetime maximums for essential coverage, including prescriptions.
In recent years, we’ve had major medical advances from CAR T-cell immunotherapy for blood cancers to a new drug for ALS, with many exciting possibilities in the pipeline. What’s the purpose of creating life-changing treatments if those who stand to benefit most never get to use them?
Courtesy of Abby Alten Schwartz
Sammie with her best buddy (2023).
Advertisement
My intention isn’t to demonise Big Pharma or private insurance — I’ve experienced the best and worst of both, and these issues are far too complex to tackle here. In countries with publicly funded health insurance, CF patients had to wait longer than those in the U.S. for access to the triple-combo drug and some are still waiting. There are no easy answers.
My path forward resides in the space between gratitude and remembrance. Like the Cystic Fibrosis Foundation and so many in our community, I am in this for life. That means advocating for every person with this disease, supporting continued research, lobbying for health insurance protections, and using my voice to share the stories of people who are working to cure this disease — and the stories of those we mustn’t forget.
Recently, it dawned on me that my daughter would be turning 27 this year. What if we couldn’t afford access to this drug? What if it had never been discovered? The realisation grabbed me by the throat.
I texted a close friend: “Sammie is less than five years from 31.” And then I broke down.
Abby Alten Schwartz is a Philadelphia healthcare writer and communications consultant for hospital systems. Her reported stories and essays have appeared in The Washington Post, Reader’s Digest, WIRED, Salon, Scary Mommy, and elsewhere. Read her work and learn about her memoir-in-progress at abbyaltenschwartz.com.
Newly released documents from the FBI reveal that there was a potential threat to assassinate Britain’s Queen Elizabeth II during her trip to the U.S. over 40 years ago.
The late Queen Elizabeth, Britain’s longest-reigning monarch, was scheduled to visit the U.S. with her husband, Prince Philip, in 1983. More than 100 pages of documents released by the FBI on Tuesday outline a serious threat made ahead of that trip and safety concerns that came up in other visits the queen made to the U.S.
Advertisement
The documents, which were posted publicly on the FBI’s website after a Freedom of Information Act request by NBC News, reveal that an unidentified San Francisco police officer received a tip about the potential plot to assassinate the queen on Feb. 4, 1983 — just a few weeks before the royal couple was scheduled to arrive in the U.S.
According to the documents, a man said that he was going to “attempt to harm Queen Elizabeth II,” and that he intended to try to kill her either while she was at Yosemite Park or “by dropping some object off the Golden Gate Bridge onto the Royal Yacht Britannia when it sails underneath.”
The documents didn’t include information on whether any arrests were made following the threat.
The man claimed that his daughter had been killed in Northern Ireland by a rubber bullet, according to the documents.
The 1983 trip to the U.S. occurred during a decadeslong period of sectarian conflict in Northern Ireland known as the Troubles. During this period, the unionists, most of whom were Protestants, wanted Northern Ireland to remain within the United Kingdom, while the nationalists, many of whom were Irish Catholics, and the Irish Republican Army wanted it to join the rest of Ireland.
Advertisement
The British deployed its military to Northern Ireland during the bloody conflict, which lasted for 30 years until a peace agreement was signed in 1998.
The FBI closely monitored the queen’s visits to the U.S. over the years with the help of the U.S. Secret Service, and security continued to be a concern.
“While [the FBI] is unaware of any specific threats against the Queen, the possibility of threat against the British monarchy is everpresent from the Irish Republican Army,” the FBI wrote in one document ahead of the queen’s 1989 visit to Kentucky.
During another visit in 1991, Irish groups organised protests at a baseball game and White House event where the queen was scheduled to appear, according to a document.
The FBI cited an article published in Irish Edition, a Philadelphia newspaper, that stated “anti-British feelings are running high” ahead of her trip.
Advertisement
The document added that while there were no threats against the queen or the president, who would also be attending the events, the statements “could be viewed as being inflammatory.”
You’re reading Love Stuck, where trained therapists answer your dating, sex, and relationship dilemmas. You can submit a question here.
Watching someone you love struggle with their mental health isn’t easy. You want to support and care for that person but they might be shutting you out or worse, it could be affecting your relationship.
This week’s reader Holly has found herself stuck between a rock and a hard place. “My boyfriend is depressed and it’s affecting our relationship,” Holly says.
Advertisement
“My boyfriend has suffered from depression for the majority of our relationship. I feel bad for saying this but it’s starting to affect me too. We live together and in the last few months the depression has really put a strain on our relationship,” Holly adds.
She continues: “His moods are always up and down, he rarely wants to go out and it’s making me question the relationship. Part of me feels like I want to leave but is that fair? What can I do?”
What should Holly do? Should she fight for her relationship and support her partner?
Co-Founder of So Synced and Relationship Expert Jessica Alderson wants Holly to practice compassion.
“While it’s important for the reader to empathise with her partner’s struggles, she should acknowledge that it isn’t easy for her, either, and she shouldn’t feel guilty about that,” Alderson says.
What would you say to this reader?
“Depression can be an all-consuming mental illness, and it’s understandable that it’s starting to affect the reader as well,” says Alderson.
Advertisement
It can be emotionally taxing to support a loved one with depression so anyone in this position should have someone to talk to.
“In addition, the reader should remember to practice self-care. This might include regular exercise, taking time to pursue hobbies, and spending time with friends and family,” Alderson adds.
She explains that if your partner is suffering from a mental illness, it’s important not to fall into the trap of trying to “fix” them.
“Providing support and understanding is very different from trying to cure someone’s depression. It can be a dangerous road to go down and may cause the “saviour” to end up with serious issues of their own,” Alderson says.
Trying to save someone in a relationship usually doesn’t work as recovery from mental illnesses such as depression or addiction often requires professional help and serious commitment.
Advertisement
Alderson tells Holly that “while supporting a partner is a natural and essential part of any relationship, it’s important that we recognise our own limitations and be aware of our own needs. There’s a fine line between compassion and self-neglect, and staying on the right side of it is key for your overall well-being.”
How can one person having depression affect a relationship?
Alderson explains that “When one person in a relationship is experiencing depression, it can have a significant impact on the dynamics and well-being of both individuals involved. Here are some ways in which depression can affect a relationship:”
Emotional strain: Depression often leads to persistent feelings of sadness, hopelessness, and fatigue. The non-depressed partner may also experience feelings of helplessness, frustration, or guilt for not being able to alleviate their partner’s suffering. If it persists, both people can end up feeling disconnected from each other.
Communication challenges: Depression can impact people’s ability to communicate effectively. The person with depression may withdraw, have difficulty expressing their emotions, or struggle to engage in open and honest conversations. This can hinder effective communication and make it challenging for the couple to understand each other.
Reduced intimacy and sexual desire: Depression often causes a lack of interest in activities that people once enjoyed, including physical intimacy. One side effect of depression is a decreased libido, which can lead to less frequent sexual activity. In turn, this can cause feelings of rejection or inadequacy which can further strain the relationship.
Role imbalance: When one partner is dealing with depression, the other partner may need to take on additional responsibilities and support them, such as cooking, cleaning, or managing finances. This can result in an imbalance within the relationship, and the non-depressed partner might feel overwhelmed or neglected as they focus their energy on supporting their partner.
Social isolation: Depression can lead to social withdrawal and a reduced desire to engage in social activities. As such, the couple may end up going to fewer events together, which can leave both people feeling disconnected from their social network. The non-depressed partner may feel guilty about attending events without their significant other and may become socially isolated.
What practical advice would you give this reader?
This is clearly not an easy situation for Holly. “Deciding whether to stay with a partner who has depression is a deeply personal choice that depends on several factors,” Alderson says.
Advertisement
Holly should consider the impact that the depression is having on her own mental health. “There’s a clear distinction between finding a situation slightly challenging and feeling completely overwhelmed or unable to cope,” Alderson explains.
“One of the most important factors to consider is whether her partner is currently taking action to address his depression or is at least open to the idea,” she adds.
If her boyfriend is committed to making changes this massively impacts how likely it is that the situation will improve in the future. Holly should also consider how compatible they are as a couple on a fundamental basis.
“While depression can strain a relationship, it’s important that she evaluates whether there are other issues that go beyond the effects of depression. This includes factors such as mutual attraction, shared values, and aligned goals,” Alderson adds.
There is no one-size-fits-all answer to whether you should stay in a relationship with a partner who has depression, as each situation is unique.
Advertisement
“Ending a relationship with someone who is in need of support can be a difficult choice to make. It’s ultimately up to the individual to weigh up all the various factors and decide what feels right for them,” Alderson says.
It may feel wrong to leave a relationship when someone is suffering from mental health issues, b01ut if it’s causing significant distress for you it isn’t selfish if it’s done for the right reasons and in the right way.
Love Stuck is for those who’ve hit a romantic wall, whether you’re single or have been coupled up for decades. With the help of trained sex and relationship therapists, HuffPost UK will help answer your dilemmas. Submit a question here.
The first time I was in China, I became one of her lost girls. As I was taken from my birth mother’s arms and placed at a nearby train station, I became a statistic ― another baby uprooted by the country’s one-child policy. At 11 months old, I was plucked from China’s embrace and placed into that of my parents. My roots began to grow in the soil of a different land.
When I was old enough to comprehend the gravity of my truth, my parents sat me down and told me that I had been adopted from China. This supposed revelation did not alter the trajectory of my life as my parents feared it might. It was fairly easy, even as a child, to recognise that I did not look like those around me, especially my parents. In fact, I found it quite awesome to be different ― to have come from a country so rich with history and culture.
Advertisement
However, the reality of living in a town with a predominantly white population is that many of its residents ostracise anyone who is different. I tried desperately to fit in with the other kids, but it became clear early on that despite my parents’ whiteness, my Chineseness would always make me an outsider.
Growing up, I listened as friends discussed which parent they resembled the most, and I grappled with the guilt that came with wishing I could participate in those discussions. I laughed along with others as they asked me to talk to them in “my language” and proceeded to speak gibberish in a way that was supposed to imitate Mandarin. For years, I didn’t know how to feel, or if my feelings were even valid. I didn’t realise that these seemingly small acts of aggression were racist and that they would grow into hatred in the future.
Courtesy of Iris Anderson
The now-abandoned train station where the author was left as a baby.
The first time I returned to China with my parents, I was 9 years old and longing for a place filled with people who looked like me. I was completely in awe of the country that created me, and this is when I first realised that I needed to embrace being Chinese. This proved nearly impossible. It was obvious that I did not belong to those who lived in China. From the way I dressed to the language that I spoke ― or couldn’t speak ― to them, I was American through and through.
Advertisement
As the trip went on, I found myself becoming increasingly disconnected from China and Chinese culture. I felt like a foreigner in a country that I desperately believed should have felt like home. This was the revelation that changed the trajectory of my life: My identity as a transracial adoptee seemed to define me everywhere I went. I was too Chinese to be American in America, and I was too American to be Chinese in China.
As I grew older, it became more common for adults to ask me how lucky I felt to be adopted from China, and I became resentful at how their questions commodified me. If I did not respond with gratitude for being adopted, it was as if a switch flipped in their mind and they saw me as a selfish girl who owes her parents everything. I left an abundance of words unsaid. To these people, this topic seemed clearly black and white: I was adopted from China after being left at a train station and should be grateful for my parents’ generosity ― for the roof they put over my head and the food they put on my plate.
Obviously, I love my parents. They have given so much to me and I would not be where I am today without them. My epiphany occurred when I realised that I am allowed to simultaneously love my parents and grieve what I lost. While transracial adoptees may be placed into amazing, loving families, it does not change the fact that their culture was stolen from them.
I have always belonged to an in-between place: not quite Chinese, but definitely not white either. The spaces and resources available to transracial adoptees are few and far between despite how large our population is, especially in the United States. My parents never hid the fact that I was Chinese, and they did the best that they could to expose me to Chinese traditions, but their efforts had their limits. Still, I am lucky to have parents who wanted and pushed for me to be connected to the country in which I was born.
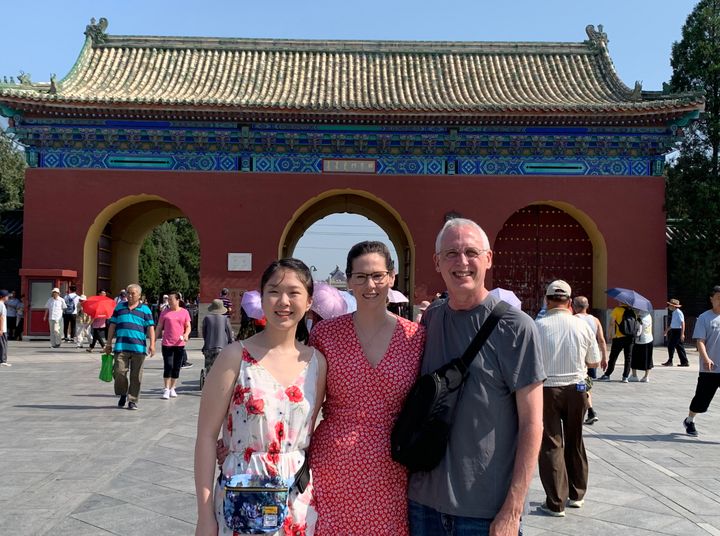
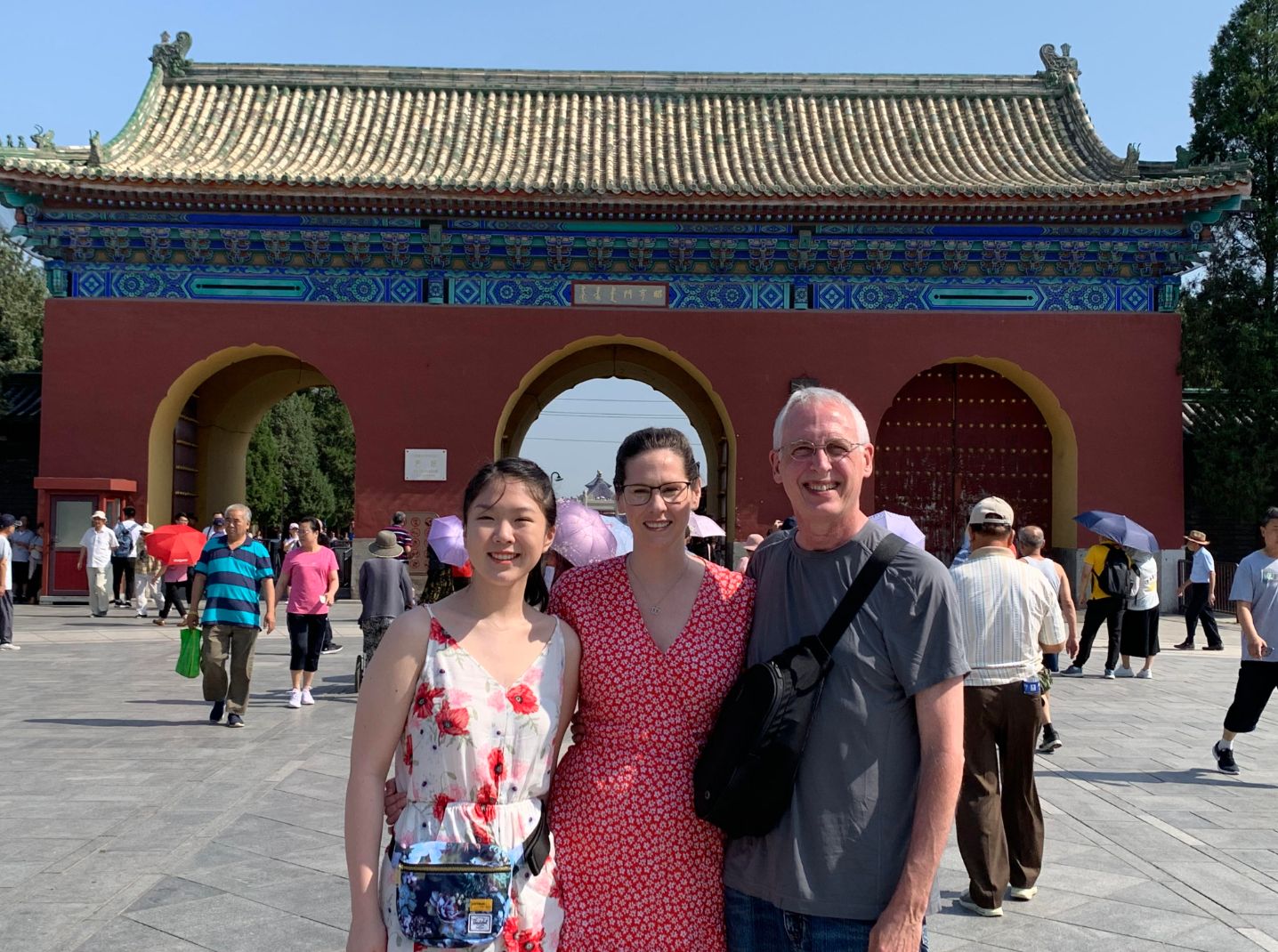
Courtesy of Iris Anderson
The author with her parents in front of the Temple of Heaven in Beijing. “I remember that day being miserably hot, but I really enjoyed being there with my parents,” she writes.
Advertisement
When I came to them about wanting to feel more connected to China and Chinese culture, they searched for years to find someone who could teach me Chinese. Unfortunately this task proved immensely difficult, so instead I began teaching myself the basics. My parents promised to take me back to China as soon as possible, especially now that I was older and could understand the importance of the trip a little bit more. They could tell I was struggling to reconcile my identities and always made sure that I knew I could lean on them for support. Unlike others, my parents never held my emotions against me and were ― and still are ― pillars of support.
The second time I returned to China, I was 15 and felt more in touch with my emotions. I wanted to build connections with other adoptees and hear their stories. This trip, which catered to adoptees from the same agency, allowed me to spend time with others who had been taken into white families.
Together, we found and created a safe environment for each other where we could talk about our experiences and vent our emotions without fear of judgment. This visit was different for me. I felt seen and heard by others who experienced the same inner turmoil that I had. Together we laughed and cried and lamented what could have been. In another life, would we have been able to meet under different circumstances?
It didn’t matter, we answered. We realised that all that mattered was what we had now, a fragmented past blended with a found family, each other included. While we didn’t all have the same goals for our return to China, we did share one: to reconcile our guilt and our curiosity. For me, I held no anger toward my birth mom for giving me up, especially when I understood the state of China and the one-child policy. But the curiosity of knowing about where and who I came from was there, and probably always will be. By the end of the trip, I cannot say that this goal was completely achieved. But while it might sound cliche, we adoptees did find each other, and in some way that was worth more to us than our original goals.
When I returned to the United States, I finished high school with a different perspective than the one I entered with. I felt able to embrace my in-between identity and reconcile the parts of me that had always felt at odds. Still, I lean on those I have found on my journey and continue to search for others who help me feel whole.
Advertisement
Courtesy of Iris Anderson
The author and the adoptee friends she made. “We were having so much fun at that point in our trip and were always asking our parents to take pictures of us together,” she writes.
All transracial adoptees deserve to have a place where they can release their emotions and feel a sense of community. While I know not all transracial adoptees will want or be able to return to their country of birth and connect with others who have shared experiences, I hope they can find another way to build a community, perhaps through local groups or online. Being able to share my thoughts, emotions and challenges ― which I worried only I was thinking, feeling and facing ― with people like me has changed my life for the better.
It has been a difficult adventure to reach a place where I feel comfortable with who I am ― Chinese, American and an adoptee ― but it has allowed me not only to deepen my roots, but also to make flowers bloom in my life today.
Iris Anderson is studying biology and psychology at Columbia University and is part of the class of 2026. She loves to write in her free time and is inspired by her personal experiences and those around her. Iris would like to thank her University Writing professor, Emily Weitzman, and her Literature Humanities professor, Taarini Mookherjee, for their support of her writing endeavours.
For many of us, loss comes with a lot of feelings of not just sadness but guilt, frustration, and even numbness. Grief varies from person to person and there is no right or wrong way to grieve. One thing that does seem to be common, especially for those of us who have lost older relatives, is feeling like we missed our opportunity to get to know them better.
In fact, according to research commissioned by KYN, innovators in later life care, 66% of Brits who have lost older loved ones wish they’d had more meaningful conversations to understand “the real them.”
Advertisement
For 29% of respondents, this was due to not spending enough time with them, for 26%, it was not knowing where to start and for 24%, they were worried about upsetting their relatives by asking about their pasts.
Researchers say that the new research “highlights one of the biggest taboos of later life – the conversation chasm between younger and older generations that leaves many never really getting to know their nearest and dearest.”
Have Meaningful Conversations With Relatives By Asking These Questions
In time for Dementia Action Week (15th-21st May), KYN and psychologist Honey Langcaster-James collaborated to create 21 meaningful questions to start conversations with older relatives.
What have you learned over the course of your life that you can pass on to me – what do you think it would be good for me to know?
Tell me about some of your earliest memories.
Where were you born and raised, and what was it like there while you were growing up?
What was your childhood like overall and what is your fondest memory from when you were young?
What were your school days like and what did you most enjoy learning about at school?
What hobbies and interests did you have, and what did you most enjoy doing in your free time when you were younger?
What is the most surprising thing you think people don’t know about you?
What was your favourite music or artist when you were growing up and why?
What has been the most interesting job you’ve ever done?
Who have you loved during your life, how did you first meet them, and how did your love story unfold?
What is the most significant historical moment you lived through or witnessed and what did you think about it all?
What was your favourite decade overall and why?
Who were your role models and who influenced you in your life and why?
Where was the most interesting place you ever travelled to and what did you make of the place?
What was the most challenging obstacle you had to overcome in your life and what did you learn from that?
What is your proudest accomplishment in life and why?
Looking back, what advice would you give to your younger self?
What’s the best book you ever read and why?
What have been the biggest changes you’ve seen throughout your lifetime?
What’s the funniest thing that ever happened in your life and what makes you laugh?
What are your hopes for the future and how would you most like to be remembered?
Emma Hewat, Head of Dementia at KYN said: “In later life, sadly it’s quite common to lose sight of people’s identity and only focus on their age or the condition of their health. People’s past experiences, current interests and future wishes are still as relevant in later life as they ever have been and it’s really important to continue to reinforce that through having meaningful conversations.”
1 in 3 People Born In The UK This Year Will Develop Dementia In Their Lifetime
According to Alzheimer’s Research UK,1 in 3 people born in the UK this year will develop dementia in their lifetime and, currently, it’s estimated that 944,000 people are estimated to be living with dementia in the UK. 52% of the UK public know somebody who has been diagnosed with dementia.
While dementia is currently incurable, early diagnosis can lead to improved quality of life and care. According to the NHS, early symptoms of dementias can include:
Memory loss
Difficulty concentrating
Finding it hard to carry out familiar daily tasks such as getting confused over the correct change when shopping
Struggling to follow a conversation or find the right word
Being confused about time or place
Mood changes
If you notice these symptoms, speak to a GP sooner rather than later.
At 32 years old, I was given 16 months to live. On an ordinary Tuesday morning in November, an ultrasound detected 12 lesions on my liver that would soon be confirmed as stage 4, incurable ocular melanoma.
It wasn’t supposed to happen. Just one year earlier, I had become a cancer survivor in 22 days. A single tumour was contained in my eyeball and a biopsy of the cells gave me the best possible outcome: There was a less than 2% chance of metastatic disease.
Advertisement
But somebody has to be the 2%.
My oncologist said I had one FDA-approved treatment option, and I trusted her. I didn’t have time to get a second opinion. In the 16 months she predicted I had left if I agreed to the treatment she suggested, I needed to get my affairs in order and explain to my precious nephews and niece why their (favourite) auntie wouldn’t live to see them get their drivers’ licenses, graduate or get married.
As he’d already been planning to do, my boyfriend Nick proposed to me on Thanksgiving, two days after my diagnosis. I had expected to spend the day in the corner of the room brooding over my fateful news and avoiding loved ones. His proposal and my new ring swept me up in a wave of hope and optimism for a future I wasn’t sure existed.
Courtesy of Katie Ortman Doble
The author on Thanksgiving Day in 2014, two days after her stage 4 diagnosis, as her then-boyfriend Nick proposed. “My nephew photobombed the proposal,” she writes.
And while I vacillated between planning my funeral and my wedding in my head, I had one crucial advantage in my new reality: My father is a doctor of internal medicine.
Advertisement
Before a drug becomes FDA-approved, it goes through the clinical trial process. For someone like me with an advanced, rare disease, clinical trials offered a better shot at buying more time, which is really all we’re hoping to do.
My father asked my oncologist about clinical trials.
“That would be very expensive,” was all she told us.
We, rightfully so, give doctors authority. They have advanced degrees. They dedicate their lives to understanding human biology, science and pharmaceuticals. I’m just a headhunter. What do I know?
If it were not for my father, who questioned the authority of this doctor, I would have blindly followed her. And I can say with certainty that had I done that, I would be dead right now.
Courtesy of Katie Ortman Doble
From left to right, the author’s husband Nick, the author, and her father/agent, James Ortman, get ice cream in New York City between scans and appointments at Memorial Sloan Kettering in 2015.
My father, whom I began referring to as my agent, spent every waking moment talking to doctors all over the country to find a glimmer of hope — something that could buy us more than 16 months.
Advertisement
He got me an appointment that December at Memorial Sloan Kettering in New York City. And so began my crash course in clinical trials (also called studies or protocols). My “agent,” fiancé (a word that tied me to a future in which I was alive) and I met with the doctor there, who explained our options.
He spoke about the importance of strategy in creating my treatment plan. Had I started on the first treatment option provided by the oncologist who diagnosed me, for example, I would not have been eligible for the clinical trial he was running.
Courtesy of Katie Ortman Doble
The author and Nick in 2016 when she lost her hair for the first time. “Nick and my nephew/godson Tommy both shaved their heads with me each time my hair fell out, as did my brothers, father and father-in-law,” she writes.
I have heard of other patients who frantically start chemotherapy upon a terminal diagnosis, only to find that made them ineligible for potentially life-saving clinical trials. When you’re given an expiration date, it’s hard to take a pause on attacking the thing that is attacking you, but this approach can mean having a matter of months versus years (or life and death).
All cancer treatments start as clinical trials, so clinical trials are essential in advancing medicine. The clinical trial process typically includes four phases focused on safety, efficacy, comparison to standard of care and the safety of treatment over time, and the majority of drugs fail in one of these phases. The estimated median cost to develop just one successful drug is $1 billion and approval takes 12 years on average. The FDA approval process itself takes six to 10 months.
Advertisement
The first five weeks of the MSK trial were packed with appointments, and as a Midwest girl living in Denver, I was secretly thrilled with the opportunity to temporarily live in a tiny, expensive apartment in Midtown Manhattan. While I worked in my company’s Midtown office, I also saw a Broadway show, went wedding dress shopping and found myself with a hideous, full-body rash from the trial’s side effects the week before my wedding.
Courtesy of Katie Ortman Doble
The author climbing a fourteener in Colorado through First Descents in 2016. “First Descents provides the healing power of adventure to young adults impacted by cancer and MS,” she writes. “I was the recipient of First Descents’ Out Living It Award in 2021.”
I was starting to understand the expense of clinical trials that my first doctor referenced. For me, the financial burden came from the airfare and lodging. I’ve been lucky to have excellent insurance through work and a job that allows me the time off. I have peers who have survived cancer only to be left six figures in debt, which leads to crippling stress, which in turn damages their health.
Those who don’t have insurance, or have astronomical deductibles, or can’t afford the financial demands that come with participating in a trial, aren’t able to get treatment that could save their lives. It isn’t fair that our health care system favours the privileged.
I spent eight months in treatment at MSK, flying to NYC monthly from Denver to pick up my medication and get scans. But by August of that year, the growth of my tumours eliminated me from the trial. Thankfully, we were ready with the next trial option.
Advertisement
This was another critical strategy introduced by my doctor at MSK that I encourage other patients to explore and understand. For someone like me, it wasn’t likely that I’d only do one clinical trial. While my doctor kept my tumours at bay, he and my dad continued conversations with doctors all over the country to be sure we had a plan B and C, in case I wasn’t eligible for plan B. We didn’t want to wait until I was eliminated from my first trial. We wanted to be ready. And since some trials and treatments might make me ineligible for others in the future, we had to be very methodical with our next step.
I participated in two trials back home in Denver over the next two years while also exploring Y90 or liver embolisation, something that was only FDA-approved for metastatic colon cancer at the time. My tumours responded really well to that therapy, buying me 3.5 years of stability and the chance to finally enjoy a delayed honeymoon with my husband.
Courtesy of Katie Ortman Doble
The author visiting her “happy place,” the Cliffs of Moher in Ireland, with Nick in 2016 after her third clinical trial.
In May 2020, substantial growth in my tumours pushed me into my fourth clinical trial at UPMC-Pittsburgh. Getting into clinical trials isn’t guaranteed or easy, especially when cross-country travel is involved. It typically includes a battery of tests like an EKG, echocardiogram and a CT scan or MRI. In my case, I had three liver biopsies in short order from three separate hospitals because each wanted its own tissue.
Liver biopsies feel like someone is taking a staple gun to your liver. Our bodies endure so much simply staving off cancer, not to mention the pokes and prods that come from treatment. The doctor also needs to see that you and your bloodwork are within the safety parameters of the trial.
Advertisement
Just as getting in isn’t guaranteed or easy, neither is staying in the trial. When you get eliminated from a trial, it’s usually for tumour growth or something else entirely out of your control. I was unknowingly kicked out of my second trial after one infusion because I was taking steroids that the doctor prescribed to combat one of the side effects. I was grateful that I continued to have options, but the volatility of it all was exhausting. The worst part was always the in between, when I didn’t have a plan and the fear of the next treatment haunted me.
In Pittsburgh, the goal of the TIL therapy was to re-sculpt my immune system with cancer-fighting cells. Enrolling was labour-intensive. There were the standard exams that deemed me eligible, plus the steps involved to create my treatment. The doctor laparoscopically removed two tumours from my liver and from those cells, grew the TIL or Tumour Infiltrating Lymphocytes. A leukapheresis extracted my white blood cells, which were then fed to the TIL, multiplying them from the millions to the billions.
Courtesy of Katie Ortman Doble
The author in her hospital room at the end of her TIL treatment in 2020. “Nick and I branded ourselves as theincreDOBLES,” she writes.
That September, I spent three weeks in the hospital receiving seven days of chemotherapy, my TIL infusion and IL-2. Because of that one time I was unexpectedly eliminated from a trial, I held my breath until the TIL hit my bloodstream. I closed my eyes and pictured the reprogrammed cells reuniting with their former tumour friends to now attack them.
I decorated the muted coloured walls of my hospital room like a dorm with my “F*CK cancer” cross-stitch, pictures of my nephews, nieces and loved ones, and pictures of my body doing adventurous things like skydiving, kayaking and jumping into the Adriatic Sea. When my hair started to fall out, Nick shaved my head and went back to the hotel to shave his own.
Advertisement
My life started to feel like a game of whack-a-mole. But I was so grateful. Through all the flying back and forth, different doctors and side effects, I was buying time I wouldn’t have had if I’d listened to my first oncologist. At the time of my diagnosis, there was only a half page of trials to explore. When I had growth in 2020, there were over three pages.
Courtesy of Katie Ortman Doble
The author with Nick and their “doghter” Alice in 2021 after the author was told she had “no evidence of disease” (NED).
I responded well to TIL, with some tumours shrinking and a few disappearing. One rogue tumour that my doctor called the “festering problem” kept growing. Naturally, I named it Uncle Fester. In September of 2021, my doctor told me he wanted to surgically remove Uncle Fester and all remaining cancer, and I eagerly obliged.
On Sept. 17, 2021, nearly seven years after I’d been given 16 months to live, I awoke from surgery to hear the words we once thought impossible: “We got it all, Katie. You are no evidence of disease (NED).”
If it weren’t for my father/agent, I wouldn’t have known how to navigate the world of clinical trials that ultimately bought me enough time to (so far) see the first of nine nephews and nieces drive his car.
Advertisement
Clinical trials are not going to be the answer for every diagnosis, but they need to be a consideration, not an afterthought. If you or a loved one gets diagnosed with cancer, talk to your doctor about what clinical trials are available. This might require getting a second opinion — which ideally is done prior to starting any treatment.
Courtesy of Katie Ortman Doble
The author and Nick in New Zealand in 2022 celebrating her NED status.
This month marks 20 months since I became NED. My doctor continues to monitor me, and I am cautiously hopeful. Of course, there’s the chance my cancer returns. My doctor hopes that the TIL in my bloodstream remains dormant in my lymph nodes and reactivates if that happens.
I haven’t had a reason to speak to my original oncologist since seeking a second opinion, but I’m almost certain she thinks I’m dead.
Katie Ortman Doble is a headhunter, stage 4 cancer survivor, patient advocate, keynote speaker and author (blog: Future Happy Self) who is currently seeking an agent for her memoir. In 2017, Katie was given the Courage Award from the Melanoma Research Foundation. She received the First Descents′ Out Living It Award in 2021 and was recently highlighted as a Medical Hero by CISCRP. She and her husband, Nick, reside in Denver with their doghter, Alice. Connect on Liinks and follow Katie’s story of survival on Instagram/Twitter @ceortman.
I’ll say it: some mourning processes are absolutely wasted on the dead.
Confessions of lifelong admiration? A chic all-black-clad gathering of your nearest and dearest? I could go for those now, TBH. And now, it seems I have another process to envy (thankfully, it’s appropriate for the living) – Swedish death cleaning.
Swedish what now?
The process, known in Swedish as döstädning, is designed to make it easy for your loved ones to pack away your stuff after you’re gone.
Advertisement
It involves simplifying your life by clearing away your old clutter, with the ultimate aim of chucking out more stuff than you accumulate.
And while cleaning is a big part of the process, Swedish death cleaning is much more of a minimalist exercise in intentionality than it is a weekend-long purge.
The goal is to have a true ‘place’ for everything in your life instead of mindlessly accumulating objects that end up being more of a nuisance than a beloved item (my enormous collection of unread books and I are trying not to feel offended).
She mentions that you should start the system aged around 65, but IMO, it makes too much sense to hold back on.
So, how do I get started?
First of all, there’s no need to get into a decluttering frenzy.
The whole point of death cleaning is to slowly ensure that you’re surrounded only by things that matter to you, so don’t toss the entire contents of your bedside cabinet away in the name of ‘living clean’.
You’ll want to start with the easy (read: massive and annoying) things first. That mattress you’ve been itching to throw out? The used-once-then-neglected paddleboard you bought during your brief ocean fixation phase? Yeah, those should be the first to go.
After all, Magnusson reckons “Mess is an unnecessary source of irritation” – so the clearing process will be easier if you chuck out the things that annoy you most first.
And you shouldn’t make death cleaning a one-off thing, either. Magnusson says that “Death cleaning is not about dusting or mopping up; it is about a permanent form of organisation that makes your everyday life run more smoothly.”
Advertisement
In other words, a one-off purge won’t cut it.
Don’t forget to include your online clutter, too
It can be tempting to limit your cleaning to the most satisfying, obvious parts of your life, like that crowded mantlepiece or the chaos in your attic.
But when it comes to Swedish death cleaning, ‘clutter’ just means anything that gets in the way more than it enriches your life, and which would be overwhelmingly annoying for someone else to clean up.
Remember, it’s about starting to sustainably shed more of life’s excess materials than you gain. So I reckon it’s about time we make a pact to delete three unflattering old selfies and blurred pocket pics for every new one we take, don’t you?
Think about what your extra stuff really means to you and others around you
Of course, this consideration has an incredibly specific application when you’re actually using it for death cleaning – in that case, it’s worth asking yourself if your daughter really has room to store your beloved grandfather clock.
But anyone who’s lived with more than two other people will know how intrusive other people’s accumulations can be. Consider whether or not your unused, spare room-consuming camping gear or cutlery drawer-dominating melon baller is as meaningful to you as it might be annoying to those around you.
In other words, gifting, donating, and selling are part and parcel of the process.
So, fellow hoarders, if you’re also growing weary of your Vague Piles of Indiscriminate Stuff, it might be time for both of us to take a lesson from the Swedes.
How much thought do you put into how you’re eating what’s on your plate? You might opt to save the best for last – we’re looking at you, Yorkshire puds! – but beyond that, the order in which you eat your food might not really cross your mind.
Well, according to some nutritionists, how we eat can be just as important as what we eat. One study shows that if you eat a meal in a specific order, you can reduce the glucose spike of the meal by 75%.
Advertisement
The concept is built around slowing down the digestion of carbs (which you have last) so as to avoid a massive rise in blood sugar.
So, without further ado, here is the order you should eat your meal (according to experts) in order to boost energy and reduce rollercoaster blood glucose levels.
First up, pack in the fibre
Scientist and author Tim Spector, author of the book Food For Life which explores the science of eating well, recommends starting your meal with fibre and a simple vinegar and extra virgin olive oil dressing – perfect for fans of veggie nibbles and dips.
‘Good’ fibres include whole grains, barley, oatmeal, beans and pulses, nuts and seeds, and fruits and veggies.
Advertisement
We all love a massive bread basket when eating out, but Spector says the quick carbs can cause a rapid increase in blood glucose levels and a high insulin response, leading to a dip in energy later.
According to the British Nutrition Foundation, adults in the UK are recommended to consume 30g of fibre a day but are currently consuming only about 20g a day on average, which shows upping your fibre intake is more important than ever.
A high fibre intake has also been associated with a reduced risk of several conditions including constipation, heart disease, type 2 diabetes and colorectal cancer.
For dieters, getting lots of fibre early in your meal can make you feel fuller and pack in lots of nutrition. Win, win!
Advertisement
Follow up with protein
Next should come your protein and fat sources. General recommendations are to consume 15-30 grams of protein at each meal, and studies show that higher intakes – more than 40g – are no more beneficial than the recommended 15-30g, so no need to pack in as much as possible, even if you are working out.
Why is protein best to eat second? “[It] slows down the release of sugar from carbohydrates into the blood stream, preventing a sugar ‘high’ and then crash – and hunger pangs,” explains TikTok creator and nutritionist, Lovneet Batra.
Save carbs for last
Potatoes, pasta and rice should be the last thing you eat. Why? Because they’re more likely to raise your glucose levels and by eating them last, you’re slowing down how fast they’re digested.
In a fascinating video, Justin (@insulinresistant1) shows how his blood sugar spikes briefly when eating rice first as part of his meal. In a follow up video, he shows how saving his carbs until last reduces the blood sugar spike.
Carbs aren’t the enemy, but for people who have issues like PCOS, insulin resistance, fatigue and type 2 diabetes, it can be helpful to make sure blood sugar is kept as stable as possible, while enjoying the deliciousness of dinner time.