New research is offering some actionable steps we can take to protect our minds from memory loss.
A large UK-based study published this week in the American Academy of Neurology’s medical journal found that physical and mental activities – such as doing household chores, exercising or visiting loved ones may help lower the risk of dementia.
The roughly 11-year study followed 501,376 people in the UK who self-reported their physical and mental activities at the beginning of the experiment: how often they visit with friends, their education level, how often they climb stairs, how they commute to work, and more.
Advertisement
The study found certain activities were associated with a lower risk of dementia. People who frequently exercised had a 35% lower risk, people who frequently did household chores had a 21% lower risk and people who visited daily with family and friends had a 15% lower risk.
And while dementia risk factors also include things that are out of our control – like ageing and genetics ― the research underscores that there are behaviours within your power to either reduce your risk of dementia or delay the condition, Dr. Scott Turner, director of the memory disorders program at Georgetown University Medical Centre, tells HuffPost.
The study does come with a few caveats: The findings are a correlation, not necessarily a direct link. Another limitation is that because people reported their own physical and mental activities, there’s always a chance that some people forgot about activities they engaged in or reported them incorrectly.
“More research is needed to confirm our findings. However, our results are encouraging that making these simple lifestyle changes may be beneficial,” study author Dr. Huan Song of Sichuan University in China, said in a statement.
Whether through physical activity, social activity or mental activity, putting your brain to work can help delay dementia onset or reduce the risk altogether.
Chores double as both a physical and mental activity (and can even sometimes be considered exercise, Turner noted). Visits with loved ones are a social activity that also requires mental stimulation, and physical activity requires mental dedication, too.
Turner said that people who develop visual or hearing problems could be at a higher risk of dementia if they don’t address the problem by getting glasses or hearing aids. When you can’t hear or see, he explained, “you’re depriving your brain of sensory input, and you need to keep your brain stimulated” to help reduce your risk of dementia.
Morsa Images via Getty Images
Physical activity is one way to help decrease your risk of dementia.
Advertisement
Physical activity has a double benefit when it comes to dementia risk
Another risk factor for dementia is diabetes, Turner notes, and there are lifestyle patterns you can follow to reduce your risk of diabetes. These include exercising, following a healthy diet and maintaining an ideal body weight throughout your lifetime.
So, not only does exercise help slash your risk of dementia, but it also helps slash your risk of diabetes, which, in itself, puts you at risk for memory loss.
It’s never too late to implement these changes
Turner stresses that no matter your age, it’s never too late to start following some of these lifestyle recommendations. And that can be as simple as doing some extra vacuuming around the house or going for a walk with your neighbour, for example.
“I recommend doing as much as possible with lifestyle [changes] to avoid and prevent dementia,” he says. “And, of course, prevention is better than treatment.”
For those who already have memory problems or dementia, Turner says lifestyle changes that require physical, social or mental activity are still beneficial. You can help slow down the progression of dementia by keeping your brain stimulated. This is why puzzles are a popular activity among people with Alzheimer’s disease.
Advertisement
If you experience any new memory problems, talk to your doctor
“If someone does develop memory problems, then they certainly should seek evaluation starting with their primary care provider,” Turner says.
He stresses that some very treatable things cause memory problems, like sleep apnea and Vitamin B12 deficiency. But any neurological changes should be evaluated so you get the proper treatment plan.
The UK is baking, and with temperatures set to top 40°C in some parts of the country, an emergency weather warning has been introduced by the government.
Let’s be honest – Brits really aren’t used to temperatures this high at home and work, so everyone is looking for hacks to make our days a bit more bearable.
But what of your windows? Should you be opening them or keeping them shut? And how about your curtains and blinds – should they be closed, too?
We asked the experts to find out.
Windows: open or shut in a heatwave?
When it’s hot, it’s our natural reaction to open the windows to get some fresh air, but is this making us hotter?
If the air is cooler outside, you should open your windows to let the air in. But when temperatures start to rise outside, keep your windows shut to avoid letting hot air in your home and making yourself warmer. If you’re not sure how to check if it’s hotter inside or outside, use a thermometer in both places.
Advertisement
Chris Nye, from Your Overseas Home, says: “It might seem counterintuitive, but if the air outside is hotter than the air in your home, keeping your windows closed could help your home stay a little cooler.”
However, at night, you might want to open them a bit. “After the sun goes down, the outside air will start to cool down,” says Dr Lindsay Browning, sleep expert at, And So To Bed. “At this point, it is a great idea to open the windows to let in a breeze of cool external air into the bedroom, helping cool the room and to provide needed air circulation.”
This works particularly well if you have windows on both sides of your room or home. Just remember to close them first thing the morning again.
Tascha Rassadornyindee / EyeEm via Getty Images
Curtains and blinds: closed or not?
If the sun shines directly into your home, you should close your curtains to try and keep rooms as cool as possible on the hottest days of the year.
“If your house does experience more sunlight throughout the day, it’s recommended you keep your curtains, shutters and blinds shut to stop the sunlight from beaming into your home,” Lucy Askew, a spokesperson for Hillarys blinds previously told HuffPost UK.
“This will keep things marginally cooler and slightly more bearable during heatwaves.”
Nye adds: “You may even want to opt for blackout curtains to keep windows covered and block the sunlight out completely.”
Should you put foil on your windows?
Putting foil on your windows is the latest heatwave hack doing the rounds on TikTok.
Sunlight usually shines through a window which increases the heat of the sun and makes your house warm. But this hack can help you limit the amount of sunlight that get into your home.
Simply roll out some kitchen foil and apply it on your windows to block out direct sunlight.
This hack is popular in America where some states experience high temperatures all year round. In the video below, @americanredcross suggest cutting cardboard and adding it to the window after you applied to the foil.
And if your home has heated up a bit too much? It may actually be cooler to get outdoors for a bit – though do avoid the hottest part of the day. And if you are heading out, stick to shady spots such as under trees or a sun parasol.
Even though irritable bowel syndrome affects 5% to 10% of people worldwide, it’s still not taken totally seriously. To someone who doesn’t have it, IBS may seem like no big deal – like a run-of-the-mill stomachache.
But for people with IBS, a condition that may present with symptoms of chronic abdominal pain, bloating, diarrhoea, constipation or some combination of these, it can quickly become what your entire life revolves around.
Advertisement
“People with IBS are often physically and emotionally exhausted by their symptoms and by repeated efforts to get answers and treatments that could help,” Dr. Lauren Tormey, a gastroenterologist at Dartmouth Hitchcock Medical Center in Lebanon, New Hampshire, tells HuffPost. “Not only can it be challenging to make a diagnosis of IBS, but symptoms can change over time, causing confusion and frustration for both patients and doctors.”
This can lead to an all-consuming cycle of avoiding trigger foods, social gatherings that involve food and drinks (so, all of them) and any situations that entail not knowing where the nearest bathroom is – along with the following things only people with IBS would understand:
1. Being so worried you’ll experience gastro symptoms, you make them come true
“I wish I could say having IBS is always in the back of my mind, but truthfully, it’s front and centre – all day, every day,” Lauren Schneider, senior PR and communications manager at Compt, tells HuffPost. “The only time I’m not worried about it is if I know for a fact I won’t be leaving home that day.”
When we’re stressed about our gut health and anticipate a flare-up or a worsening of symptoms, it sends signals from our brain to our gut, which can actually affect our digestive system. The result? Tightened abdominal muscles, colon spasms and an uptick in discomfort.
Advertisement
“The stress associated with the fear of experiencing IBS symptoms can even result in an inability for the body to properly digest food,” Dr. Vanessa Méndez, a board-certified gastroenterologist and founder of Planted Forward, tells HuffPost. “This can lead to bloating and diarrhoea or even a slowing down of the digestive system that triggers constipation.”
2. Eating or drinking something spontaneously – and immediately paying for it
With IBS, because of the hyper-responsiveness of the enteric nervous system (the part of the nervous system located in our digestive tract), symptoms can often be unpredictable. This means turning down the chance to try a new menu item at a restaurant, or cocktails at happy hour, so as to not risk an attack of symptoms.
For people who have never dealt with IBS, these boundaries might seem like overkill. But they can mean the difference between enjoying time spent with others, or being so focused on masking your symptoms you miss out on the experience (or spend the bulk of the experience in the bathroom).
“That one scoop of ice cream is enough to make me feel like I’ve had food poisoning,” Abi Cowell, a vegan food blogger, tells HuffPost. “Will it kill me like a food allergy would? No. But it will cause an awful lot of pain and misery.”
3. Socialising is filled with mental – and intestinal – anguish
“Having IBS and socialising is filled with emotional landmines, especially when meals are involved,” Lindsay Barnes, media relations manager at Evoke Kyne, tells HuffPost.
Advertisement
There’s the frustration of people not understanding that needing to go to the bathroom means you need to go now. The fear of entering the dating world and having to explain why you go so much. The awkwardness when you’re having a good time and suddenly need to make a run to the loo.
“When you just want to sit down and have a normal meal, whether by yourself or with family and friends, these things can be emotionally exhausting,” Tormey says. “The pain experienced by individuals with IBS is in part due to visceral hypersensitivity.”
Visceral hypersensitivity is pain or discomfort coming from internal organs (like those in the abdomen), under circumstances that wouldn’t normally be painful (like eating or during a bowel movement).
The nervous system experiences these sensations and communicates them to the brain for processing via the gut-brain connection.
“Food – eating it, even thinking about it – regardless of the food type, stimulates normal digestive function and can therefore result in pain in IBS,” Tormey says. “Sometimes eating is accompanied by the immediate urge to have a bowel movement because of a heightened stomach-colon reflex.”
Advertisement
Putting food or fluid in the stomach sends a signal via the nervous system to the colon. The colon understands this as a stimulus to empty whatever waste is there – and doesn’t care if you’re mid-sentence on a first date.
10’000 Hours via Getty Images
Social outings, like dates or meals with friends, can cause emotional and physical discomfort.
4. Changing so many ingredients in a recipe or food order, it becomes a different meal
The average person can control the effects of what they put into their body, and can adapt to food-centric situations, because their sensitivities to certain foods remain relatively consistent and clear-cut.
“I don’t have that luxury,” Barnes says. “I have absolutely no control over my body anymore – I can be as mindful as possible and work really hard on my diet, but at the end of the day, my gut controls my body now, and not in a good way.”
Food intolerances are common in IBS, and dietary modifications can help manage symptoms for some people. But for others, “visceral hypersensitivity and abnormal gut-brain communication can cause flare-ups to happen anyway, despite watching what you eat,” Tormey says.
Advertisement
“And who knows how long the flareup will last?” Barnes said. “A half hour? Two hours? The rest of the day?”
5. Mapping out where every public bathroom is before you leave the house
When Schneider leaves her home, she’s always planning – always conscientious of where she can find a restroom if she needs to stop. “If I’m going to be driving somewhere without quick access to a bathroom, I won’t eat before my trip,” she says. “I’ll wait until I get there.”
These coping strategies are actually pretty common, and can be a normal response to a situation that’s outside of our comfort zone, even for people who don’t suffer from IBS.
“When anxiety levels are high in a situation such as traveling, your digestive processes can get dysregulated,” Méndez says. “During stress, the brain sends signals to the gut that influences motility and digestion, which can lead to diarrhoea or constipation.”
Because the gut is constantly at work, the brain typically filters out the nerve signals it sends (paying attention and responding to some in order to regulate gut activity, while not focusing on others). Normal gut-brain communication can go wrong when something disturbs the nervous system or the brain for a long period of time – like when traveling, working a stressful job or rushing to get errands done.
Advertisement
“In these circumstances, the brain perceives stronger signals from the gut, and even the mildest stomach cramp can immediately trigger the brain to start worrying about the potential for worsening pain or a bowel movement coming on,” Tormey says. “The brain subsequently sends inappropriate signals back that disrupt gut function and can worsen symptoms.”
As a result, you might find yourself doing the same as Schneider: scouting bathrooms on your route or delaying meals.
6. Maintaining excuses for why you’re taking so many bathroom breaks
“Something I want others to understand about how IBS impacts my life is the daily secrecy and diversions that surround my use of the bathroom,” Amanda Dexter, 36, tells HuffPost. “There’s a lot of sneaking (multiple) trips to the bathroom or making excuses as to why it took you so long.”
Eating food and having bowel movements are essential to our survival – and across cultures, food is social and often enjoyed and shared with others. But unless you’re potty training a toddler, bowel movements aren’t exactly a typical subject of dinner-table conversation.
“These aspects of daily life pose regular challenges for those with IBS,” Tormey says, and can lead to a loss of enjoyment around food, a fear of eating and even disordered eating habits, such as skipping meals to avoid needing to use the bathroom.
Advertisement
If more people were to open up about their own horror stories, Dexter believes it would help alleviate the unnecessary embarrassment that many people with IBS feel. “Commiseration can go a long way into helping IBS sufferers not feel so alone,” she says.
7. Having flare-ups so exhausting, you need to take the rest of the day off
IBS is a disorder of “dysmotility,” meaning that movement of food, fluid and waste through the gut is altered.
“This leads to irregular bowel habits (diarrhoea, constipation or both),” Tormey says. “You might spend a lot of time in the bathroom, either having bowel movements, trying to have a bowel movement or dealing with pain around the time of bowel movements.”
It’s not uncommon for people with IBS to miss days of work or school because of these exhausting, intrusive symptoms – only to be further stressed out over the resulting lost productivity and wages.
“There have been times where I feel so emotionally drained and frustrated that I’ll just cry in the bathroom,” Barnes says.
Advertisement
PixelsEffect via Getty Images
Flare-ups can be so painful and taxing, it’s hard to motivate yourself to leave the house.
8. The relief of knowing you don’t have anywhere to go that day
For Schneider, being able to work from home has alleviated much of the anxiety associated with her condition. She’s able to eat more intuitively and with a bathroom always nearby.
“Work trips are a little difficult, especially when the whole group goes out to dinner,” Schneider says. “That’s when I just resort to my old ways, and either barely eat or only eat my tried-and-true few things that won’t upset my stomach.”
Because IBS symptoms can be intermittent and unpredictable, varying in both nature and severity, the condition can leave you with a great deal of uncertainty and anxiety about what might happen outside the home.
“To compound matters, there’s a well-established recognition that the central nervous system, or brain, also has a significant role in regulating not only gastrointestinal motility, but sensation – from both an unconscious and a higher emotional level,” Dr. Brooks Cash, professor of gastroenterology at the University of Texas McGovern Medical School, tells HuffPost.
Advertisement
This typically leads to people with IBS becoming hyper-vigilant about their symptoms, and trying to be as ready for them as possible – including doing everything in their power to avoid potential triggers.
“Sometimes these triggers are absolutely accurate, and other times they’re merely innocent bystanders,” Cash says. “Either way, we often see patients changing their lifestyle, daily activities, diet, habits and social activities for the sake of avoiding them.”
9. Losing count of how often you’ve been told your IBS symptoms are all in your head
Schneider has done what’s recommended to treat IBS. She’s seen doctors, done the tests. The endoscopy and colonoscopy didn’t show anything helpful – just that she also has gastro-oesophageal reflux disease.
“I’m on an SSRI, so it isn’t anxiety-related, like one doctor so unhelpfully assumed,” she says. “She literally said to me, ‘Well, nothing’s shown up in your bloodwork or other tests – you have IBS-D but it’s probably all in your head.’ Thanks, super helpful.”
After being poked and prodded enough, Schneider gave up. “I’m tired of advocating [for] myself to doctors who won’t listen and paying co-pays that are essentially a waste of money to hear the same things over and over.”
Advertisement
While doctors don’t have an IBS biomarker to test for, there are formal diagnostic criteria for IBS called the Rome IV criteria.
“To make a diagnosis of IBS, patients should meet Rome IV criteria and not have any other ‘alarming’ signs such as blood in the stool, unintentional weight loss or new onset symptoms over the age of 50 without prior colon cancer screening,” Tormey says.
These criteria must be fulfilled for the past three months, with symptom onset at least six months prior to diagnosis. “IBS should then be sub-classified by the predominant bowel pattern – such as IBS-C, or IBS with constipation – which helps guide treatment,” Tormey says.
A diagnosis of IBS can be made confidently after a detailed history, a complete physical exam and a few thoughtfully selected diagnostic tests to evaluate for conditions that can present with similar symptoms.
So if your doctor implies – or straight-up tells you – your symptoms are all in your head, Méndez encourages you to get a second, third or even fourth opinion. “You know they’re not in your head and that IBS is a very real condition,” she says. “In fact, IBS is the most common functional digestive disorder. If you have symptoms, please keep seeking help until you find a healthcare provider you trust.”
Just so you know, HuffPost UK may collect a share of sales or other compensation from the links on this page if you decide to shop from them. Oh, and FYI — prices are accurate and items in stock as of time of publication.
It’s likely you’ve never heard of acrochordons, but you’ve probably dealt with them. In fact, they’re so common that over 50% of adults will experience them at least once in their lifetime. Better known as skin tags, acrochordons are small growths of extra skin that, while harmless, are no one’s favourite feature.
Advertisement
Health care costs are higher than ever and skin tag removal typically isn’t covered by insurance, since it’s an unnecessary procedure. These days, there are a wide array of skin tag removal products you can purchase to cut these costs considerably ― but, ew? Is that such a great idea? Just how safe are these treatments, and is skin tag removal better left to the professionals?
Doctors’ thoughts on skin tag removal may surprise you
“Do you need to go to your doctor every time you have a skin tag you want removed? Not always,” says Dr. Jaimie DeRosa, a board-certified facial plastic surgeon and founder of DeRosa Center Plastic Surgery & Med Spa in Boston. “When I was little, I remember my dad (who was a doctor) pulling his skin tags and snipping them off.”
Thankfully, there are less extreme at-home treatment options today. While none of the medical professionals love the idea of at-home skin tag removal, they do have some safer at-home ideas to try. However, there was one caveat.
“If the lesion is large or is causing pain, bleeding or discomfort, it should be removed by a healthcare provider,” says Dr. Alexander Zuriarrain, a board-certified plastic surgeon with Zuri Plastic Surgery in Miami. When in doubt, he stresses, please see your doctor.
Advertisement
Catherine Falls Commercial via Getty Images
For an idea of what skin tags look like, think about the growths on these potatoes.
If these characteristics do not apply to your skin tags, then you can consider trying these DIY recommendations below.
The household remedies that people often try
First, let’s address some of the household remedies that friends may have suggested to you. While the ones listed here are safe to try, keep in mind there are no studies that prove they actually work.
“A natural remedy that a patient introduced to me is using banana peel on skin tags. It is unknown what chemicals are in the banana peel that helps with skin tags,” says Dr. Elaine F. Kung, a board-certified dermatologist based out of New York City and founder of Future Bright Dermatology. “It has been postulated that there are antioxidants and enzymes that may be helpful.”
Nandi Wagner, the lead aesthetician at Gilded Ritual, a high-end salon in New York City, is familiar with this method, too. “Some homeopathic remedies for skin tags include applying small amounts of diluted tea tree oil, apple cider vinegar or even banana peels to the skin tag,” Wagner says.
Advertisement
DeRosa had similar advice and also suggested crushed garlic may work. She explains how to try this remedy at home: “For any of these topical treatments, wash the skin tag and surrounding area, then apply the topical of your choice to the tag, and cover with a bandage overnight. Repeat this treatment until the skin tag dries out and falls off, and stop its use if the area becomes irritated.”
But if you want a solution that’s more proven, keep reading.
Lotions with acid
“For tiny, just barely noticeable skin tags, you can try using a lotion with keratolytic ingredients over several months. In other words, lotions with AHA, BHA (salicylic acid), or lactic acid may help chemically ‘exfoliate’ the tiny little tags,” Kung suggested.
Check your medicine cabinet, as it’s possible you have products with these ingredients at home.
At-home ligation
A somewhat scarier option is to cut off the skin tag’s blood source by tying up the base of your skin tag, a process known as ligation. This will take a few days, but it’s a common method for at-home removal. While this procedure may be somewhat uncomfortable, it should not be painful. If it is, that’s a good sign to visit your doctor for removal instead.
“Ligation is another method to remove unwanted skin tags. Ligation works by cutting off the blood flow to the skin tag, causing it to fall off,” Wagner says. ”There are several [over-the-counter] ligation pens that deploy a small silicone band around the base of the skin tag, cutting off its circulation. After about five days, the skin tag generally will dry up and fall off.”
There are numerous ligation tools available online. One of the highest-rated ligation kits on Amazon is this Tag Band Micro Skin Tag Removal Kit, with a rating of 4 stars from more than 12,000 reviews.
Advertisement
Freezing them off
The “most effective and safest way” to remove skin tags, in DeRosa’s opinion, is with cryotherapy. “Cryotherapy is the use of a super-cold gas (nitrogen is the most commonly used) to essentially shrink and kill the blood supply to the skin tag. At-home cryotherapy kits vary, so just look for those that can get you the coldest settings,” DeRosa explains. This means around -15 to -50°C
DeRosa suggests Compound W Nitrofreeze, even though its original intended for wart removal. She said it gets cold enough for skin tag removal. And she means cold – the freezing temps this pen produces can lead to some initial stinging and burning during treatment. Also available on Amazon is Cryotag Skin Tag Remover, which has 11,457 reviews and a 4 star rating.
Since news of the overturning of Roe V Wade broke on Friday, ending the constitutional right to abortion in the US after almost half a century, abortion rights activists have galvanised, and social media efforts have amplified.
You may have seen posts alluding to the fact that a woman can only foster one full pregnancy a year, while a man can impregnate multiple people in a day, should he have the opportunity. And the solution often suggested: vasectomy, the surgical procedure that cuts or seals the tubes that carry a man’s sperm.
Advertisement
Amid so much anger around the policing of women’s bodies, the impulse to suggest that men’s bodies should also be policed is understandable.
In a world of reduced abortion access, where women are left either to manage birth control or carry their babies to full term, people are once again suggesting we shift the onus to men in the form of mandatory vasectomies.
You wanna know what prevents abortions? Vasectomies.
— 🖕🏻Aunt Crabby Calls Bullshit 🖕🏻 (@DearAuntCrabby) June 25, 2022
In fact, this view has been circulating on social media for a while now. And while many people are probably not being literal in their calls for vasectomies, it speaks to the widespread rage over moves to control bodily autonomy.
However, many people are pointing out the flaws in the argument.
Vasectomies aren’t an ‘alternative’ to abortion
This suggestion has basic logistical failings, as PHD researcher Georgia Grainger, from the Centre for the Social History of Health and Healthcare in Glasgow, has pointed out in a Twitter thread.
As a historian of vasectomies, Grainger, aka @sniphist on Twitter, stresses that the procedure is not an alternative to abortion.
This is because women will still need terminations, she says, both of wanted and unwanted pregnancies, regardless of vasectomies and other forms of birth control.
Nor are vasectomies a failsafe form of birth control – and when in rare cases they do fail, it’s not usually obvious until the pregnancy is identified, she says.
Advertisement
If the pregnancy is a wanted pregnancy but is either ectopic or otherwise not viable or dangerous, then a vasectomy explicitly cannot prevent that – they were wanting to be pregnant, it’s a biological mishap and needs to be treated with abortion.
If it’s caused by failed birth control, then… Vasectomies can fail too! It’s unlikely but absolutely possible. Sometimes the vas deferens heals itself years later. And there’s no way to know, unlike a split condom or missed Pill, so no Plan B.
In her thread, Grainger also highlights that even if someone had insisted they’d had the surgery, could you trust that they really had?
Especially, in the case of abusive relationships or sexual assault, why would someone who doesn’t respect consent take up an invasive surgery for the benefit of someone else?
Forced sterilisations are deeply problematic
Grainger stresses this important historical point. Forced sterilisations have been trialled as several points during history and they enforce eugenics, she says. The policy has predominantly been targeted at minority groups to stop them from procreating.
Advertisement
In US history, indigenous Americans, Black and Latinx people, incarcerated peoples, and poor communities endured forced sterilisations.
These groups were targeted throughout the 20th century, with nearly 70,000 people forcibly sterilised (and not just men, an overwhelming amount were working-class women of colour).
If you think a “mandatory vasectomy til men prove they can be a father” is even a fun thought experiment, I recommend you go and read up on eugenics. Plus, that inevitably becomes “mandatory IUDs for women” too, which again, has happened in recent US history.
Germany also has a history of coercive sterilisation, having sterilised disabled people, institutionalised people, and even alcoholics. In Nazi Germany, the Hereditary Health Court also known as the Genetic Health Court, was a court that decided whether people should be forcibly sterilised.
Grainger is not the only one to point out these troubling historical precedents.
i am BEGGING other white people to stop talking about mandatory vasectomies as if Black and Indigenous peoples haven’t been subjected to centuries of involuntary sterilization. there are other ways to discuss contraception and pregnancy prevention that don’t invoke eugenics.
forced sterilization of cis-men would ultimately impact Black and brown men the most as all of these restrictions always target the most vulnerable of our population
hi this is called eugenics! what is so hard for people to understand about this? BODILY AUTONOMY FOR EVERYONE, NOT PUNISHMENT. pic.twitter.com/kLZomQGkQB
— Elly Belle 🔮 (famously not a woman) (@literElly) June 26, 2022
Bodily autonomy for all, not some
People have also pointed out that if we want better rights and autonomy for women and people who can get pregnant, this has to mean protecting these rights for everybody
Do we really want men to face the same bodily scrutiny applied to women – and for men who chose not to go through the procedure to be vilified?
Advertisement
Nor does the vasectomy vs abortion binary do much for trans and nonbinary people who also need access to abortions, and are often excluded from discussions of these human rights.
The pro-choice movement is all about bodily autonomy and protecting everyone’s right to make decisions about their own bodies
As the debate continues, Grainger’s insights have gone viral on Twitter, amassing more than 75,000 likes.
But, as she pointed out in her own thread, she is still pro-vasectomy, as long as they’re for the right reasons and for people who genuinely want them.
Ultimately, we shouldn’t pit vasectomies against abortions, she says. Abortions will always be needed, whether because the pregnancy is failing, the pregnant person is at risk, because there wasn’t consent to the sex in the first place, or simply because the pregnant person doesn’t want children.
Advertisement
So next time you see calls for mandatory vasectomies or are temped to make one yourself, remember that it’s not as straightforward as it seems.
People who remain on the waiting list for health treatments are being asked whether they are prepared to travel to receive treatment.
NHS England is set to “virtually eliminate” the list of those who have waited more than two years for treatment, the chief executive has said, as patients are given the option to be treated more quickly at hospitals in different parts of the country.
Advertisement
Of course, this plan will do little to help those without access to transport, those who need to juggle healthcare alongside care responsibilities, and those on zero hours contracts or self-employed, who need to take limited time off work to avoid pay losses.
The number who have waited for two years or more to receive treatment has fallen from a peak of 22,500 in January to 6,700, after the Covid-19 pandemic caused waiting lists to mount.
People who remain on the waiting list are being asked whether they are prepared to travel to receive treatment. More than 400 have agreed, with 140 booked in for surgery at a different hospital.
NHS chief executive Amanda Pritchard said: “As part of the biggest and most ambitious catch-up programme in NHS history, staff are now on track to virtually eliminate two-year waiters by the end of July.
Advertisement
“But the NHS will not stop here, from delivering one million tests and checks through our newly rolled-out community diagnostic centres to new state-of-the-art same-day hip replacements, staff are constantly looking for new and innovative ways to treat patients quicker, especially those who have been waiting a long time.”
The NHS has said it will cover travel and accommodation costs to patients “where appropriate”.
Three patients who had been waiting to receive treatment at University Hospitals of Derby and Burton NHS Foundation Trust went on to receive treatment at Northumbria Healthcare Foundation Trust more than 100 miles away, with a further two booked in.
Meanwhile, South West London Elective Orthopaedic Centre has treated 17 patients from the South West of England, and a further 11 are expected to receive treatment in the coming weeks.
Patients who opt to wait longer, or patients in highly-specialised areas that may require a tailored plan, however, will not necessarily have been treated by the end of July, the NHS warns.
The fall in waiting list numbers comes after the busiest ever May for emergency care, with 2.2 million A&E visits and almost 78,000 of the most urgent ambulance call-outs.
Advertisement
Pritchard added: “One of the benefits of the NHS is that hospitals can work together to bring Covid backlogs down together and so if people can and want to be treated quicker elsewhere in the country, NHS staff are ensuring that it can happen.
“Once again, NHS staff are demonstrating the agility, resilience and compassion that shows when they are given the tools and resources they need, they deliver for our patients.”
Health Secretary Sajid Javid said: “Innovations like this are helping to tackle waiting lists and speed up access to treatment, backed by record investment, and there are over 90 community diagnostic centres delivering over one million checks and scans in the last year.”
Saffron Cordery, interim chief executive of the NHS Providers organisation, said the health service is “nearing the target” of clearing the backlog of all people who have been waiting for more than two years for hospital care.
She told BBC Breakfast: “The NHS is doing incredibly well and we are seeing those figures coming down significantly week by week. I never like to say ‘Yes, it will definitely happen’, but I think it’s testament to the hard work of trust leaders up and down the country that that we are nearing that point.”
Advertisement
Asked abut the call for more nurses, she said: “We’ve known for a very long time that workforce is a significant challenge.
“I think one of the things we have to remember is that the challenges we are facing now, post-pandemic, were there before the pandemic and the pandemic has simply exacerbated them.
“So we’ve got funding challenges that have come from a decade’s worth of a funding squeeze; demand was already going up before the pandemic; we had challenges in terms of social care which we’ve got now and they are increasing significantly.
“But we’ve also got this workforce shortage, which is incredibly serious.
“We’ve called on the Government to establish a fully funded and costed long-term workforce plan so we can sort this out once and for all but we know there are big challenges there across the nursing workforce, across the doctor workforce and other parts of the NHS staffing structure.”
Polio, which was officially eradicated in the UK in 2003, can cause paralysis in rare cases and can be life-threatening. Public health officials have declared a national incident while the latest traces are being investigated.
Polio is caused by a virus that spreads easily when an infected person coughs or sneezes, according to the NHS. It can also be caught from food or water that’s been in contact with the poo of someone who has the virus.
So far, it’s unclear how many people may be affected by the new outbreak, but being fully vaccinated will protect you. Here’s how to check if you (and your kids) are up to date with jabs.
When do people usually receive the polio vaccine?
The polio vaccine is given on the NHS when a child is eight, 12 and 16 weeks old as part of the 6-in-1 vaccine. It is given again at three years and four months old as part of the 4-in-1 (DTaP/IPV) pre-school booster, and at 14 as part of the 3-in-1 (Td/IPV) teenage booster. The teenage vaccine is given routinely in secondary schools.
All of these vaccines need to have been given for a person to be fully vaccinated, though babies who have had two or three doses will have substantial protection.
Latest figures show that by the age of two in the UK, almost 95% of children have had the correct number of doses. However, this drops to just under 90% in London. When it comes to the pre-school booster, just 71% of children in London have had it by the age of five.
How to check if you’ve had the polio vaccine
All immunisation records are linked to your unique NHS number, which is assigned to you at birth.
You may be able to see your full health records (including your immunisation history) via the NHS app or NHS online portal, if you’ve already registered for full online access.
You’ll need to register with your GP surgery for online access to see your full record. If you only downloaded the NHS app to see your Covid travel pass, for example, the basic profile only shows your Covid vaccines, medicines and allergies – not your full medical history.
There’s a portal on the NHS website which details further instructions on how to register for full online access to your records. But something to note: this service works alongside GP surgeries and is not yet available in all areas of the UK.
If you’re having trouble accessing your records online, or your surgery does not offer this service, you’ll need to contact your GP to enquire about your polio records via email or telephone.
A polio vaccine will not be labelled as ‘polio’
When you do access your records, don’t panic: a polio vaccine is rarely labelled with the name ‘polio’.
On Twitter, GP and broadcaster Dr Ellie Cannon shared the labels to look out for:
Sleep, O sweet sleep, where art thou? Some nights it’s impossible to doze off, all the world’s thoughts heavy on your eyelids.
So whenever I see a trick or vital TikTok that promises a hack to make you fall asleep instantly, I’m hooked.
Advertisement
This week, I came across a content creator who goes by @YoungerYouDoc, teaching people “how to become the youngest version of themselves”.
In one video, he demonstrates how rubbing your wrists for two to three minutes can help you nod off. This is because a spot on your wrist provides one of several pressure points for sleep, according to reflexologists.
“There are four acupressure points starting at the pinky side of the wrist crease and moving up the inner forearm,” Dr Shari Auth, chief healing officer and co-founder of WTHN, told Bustle.
“They are good for insomnia and are excellent to rub at bedtime. These points are commonly used by acupuncturists to treat sleep, palpitations, and mental health issues such as depression and anxiety.”
Advertisement
So, for the last two nights I’ve tried the trick to see how it affects me. And unfortunately, it didn’t help at all.
Perhaps I had the wrong point (I watched a video about pressure points and it seems I did rub the suggested area). But what stopped me from falling into a slumber was being conscious that I was rubbing my wrist.
Before I fall asleep I like to be as still as possible, so I think for me it felt unnatural to keep rubbing for a few minutes.
I also switched hands in case one wrist was more effective than the other. But after doing it for a while, my wrist started getting warm and I decided to give up.
Advertisement
I also didn’t sleep very well and it took me longer to fall asleep than it would usually (though that might be unrelated).
In another viral video, he explained how his two-minute method was adopted by military personnel who often sleep in rough conditions.
It consists of incrementally relaxing your body, then imagining a warm light travelling through your body, while focussing on your breathing. Then you clear your mind of all stresses.
To do this, Agustin advises imagining one of two scenarios; the first is lying in a canoe in a calm clear lake, with a blue sky above you. The other is lying in a velvet black hammock under a pitch black sky.
Any time your thoughts try to distract you, repeat the words ‘don’t think’ 10 times.
Sounds simple enough, right? Well, Agustin explains, you’d need to do this every day for six weeks to see it work effectively enough to fall asleep within two minutes.
It might sound tedious, but it might be worth it in the long run.
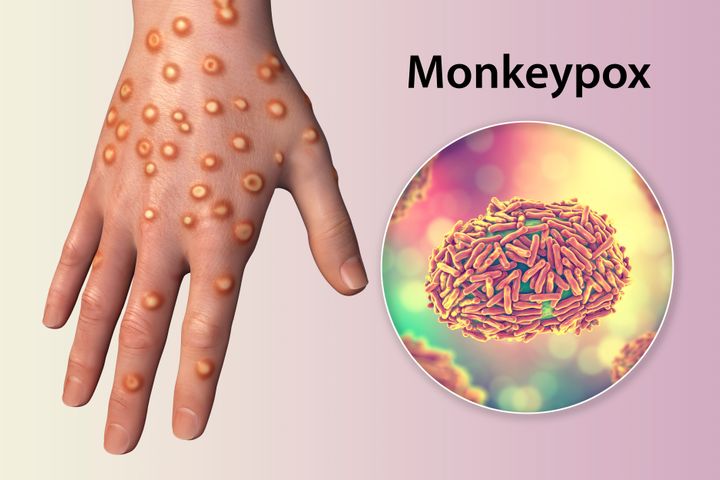
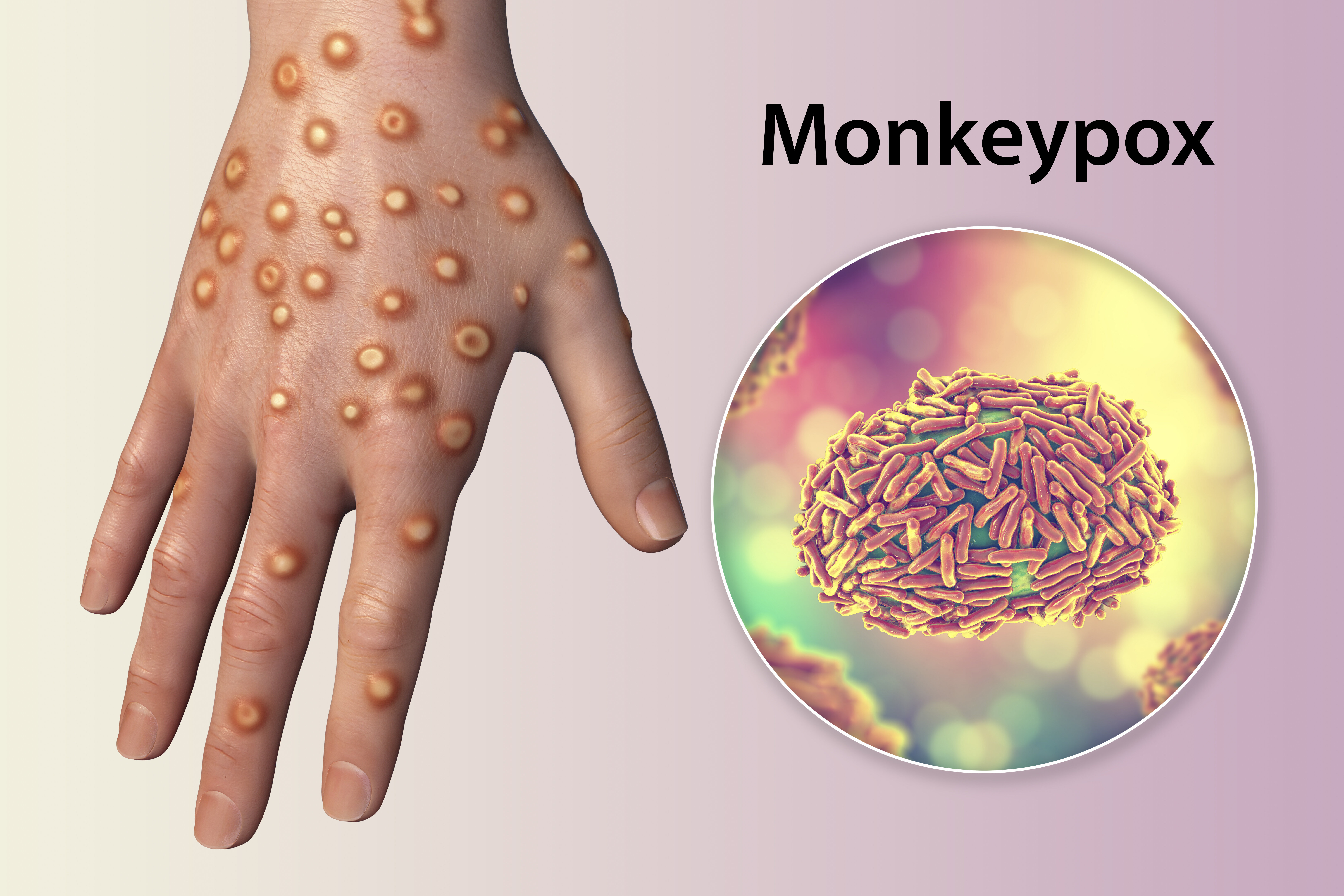
People who are at highest risk of catching the monkeypox virus will soon be offered a vaccine in an effort to reduce transmission.
The UK’s Health Security Agency (UKHSA) has revealed that some men who have sex with men will soon be offered the Imvanex jab – originally designed to treat smallpox – to curb the largest recent outbreak outside of Africa.
The World Health Organisation (WHO) believes that the outbreak stemmed from sexual activity by men at raves in Spain and Belgium.
More than 99% of the current 793 reported UK cases are among men, most of whom identify as gay or bisexual.
Anyone – regardless of sexual orientation – is at risk of contracting the virus if they are in close contact with someone infected with monkeypox, or infected clothing or bedsheets.
Advertisement
But, men who have sex with men and who have multiple partners are considered at the highest risk – this includes those who take part in group sex, or go to venues where sex occurs on the premises – due to the origins of this particular outbreak.
The agency said data suggests there are higher levels of transmission “within, but not exclusive to, the sexual networks of gay, bisexual and other men who have sex with men”.
UKHSA’s head of immunisation Dr Mary Ramsay said: “By expanding the vaccine offer to those at higher risk, we hope to break chains of transmission and help contain the outbreak.”
Is this the first group to be offered the vaccine?
No – vaccines were offered to health workers who look after monkeypox patients as well as cleaners disinfecting areas which may have been exposed to the virus.
Close contacts of confirmed cases were also offered the vaccine.
NHS England will soon provide more details about how those who are eligible can receive a jab, although people are advised not to approach the NHS until contacted.
Advertisement
Vaccines have never been used in Africa to impact monkeypox, even though it is endemic in some countries.
It’s also worth noting that this vaccine is not designed specifically for monkeypox. Although Imvanex was used to eradicate smallpox worldwide, it has been found to be 85% effective against this current virus.
KATERYNA KON/SCIENCE PHOTO LIBRARY via Getty Images
Hand of a patient with monkeypox infection and close-up view of monkeypox virus particles, computer illustration
Does this news mean there’s cause for concern?
Well, it’s unclear at the moment.
No deaths outside of Africa have yet been reported from this outbreak, although confirmed cases have suffered from fever, swollen glands and a rash which develops into fluid-filled lumps.
There are currently 793 cases in the UK out of more than 2,100 cases around the world – far lower numbers compared to when the Covid vaccine rollout first began.
Advertisement
However, the Joint Committee on Vaccinations and Immunisations (JCVI) supported the decision to start handing out the smallpox vaccine. This panel advised the government to start its vaccination programme for Covid last year.
The WHO has described the outbreak outside of the continent as “unusual and concerning”, and is considering declaring it a global emergency.
Dr Ramsay warned: “Although most cases are mild, severe illness can occur in some people, so it is important we use the available vaccine to target groups where spread is ongoing.”
Professor Paul Hunter from University of East Anglia’s school of medicine also told Sky News that vaccination was “the right thing to do”.
He added: “What we have seen with monkeypox is a significant and continuing increase of the second wave despite control measures having been in place for a few weeks.
Advertisement
“So it is certainly looking like the current strategy of ring vaccination is not working.
“This is probably down to difficulties in identifying cases and their contacts rapidly enough, possibly due to stigma.”
He suggested that “we should be ready to start offering the vaccine to female sex workers” as well, because the virus does not discriminate by sexual orientation or sex.
You’ll have to do a PCR test similar to the Covid test. For monkeypox, it involves three swabs, two for the skin, and a throat swab.
You are still allowed to travel on public transport if you suspect you’ve caught the virus, but wear a mask and cover any lesions.
If you need to isolate, do not share a bathroom if you can avoid it and isolate in one room. Make sure not to share bedding or towels, avoid contact with your pets and have no sexual contact.
Try to avoid other communal spaces, too, such as the kitchen.
Remember being 21, drinking whatever you could get your hands on (i.e the cheapest booze) with nary but a piece of toast to line your stomach? And somehow the next morning, you were still fine to make it to uni, or work, or just a day of youthful hedonism?
Well yeah, at some point that changes and out comes the hangover from hell to humble you.
There’s something about getting older that makes you more likely to experience the dreaded hangover sickness – headaches, a raging stomach, nausea, and other fun things.
Advertisement
And now, researchers have put a number on when you’re most likely to feel rough. And sorry 34-year-olds, it’s not looking good.
Greeting cards company Thortful carried out a survey of 2,000 people and found that post 34, you’re likely to start getting raging hangovers. And after 35, the dreaded after effects of drinking seem to last two days.
The survey found that we only start realising our boozy limits at age 37, while a year later is when people feel ‘too old’ to go out-out.
Advertisement
You’d think that as we get older, and thus more acclimatised to drinking, our bodies would be used to it. But actually it’s kind of the opposite.
“This means there are more toxins in our bodies for longer as they’re broken down more slowly into carbon dioxide and water,” Booker previously told HuffPost UK.
But before it can get to the CO2 and water stage, alcohol is broken down by the liver into a number of different substances, including the compound acetaldehyde. Dr Niall Campbell, consultant psychiatrist at Priory’s Roehampton Hospital, explained that as we age, our ability to metabolise acetaldehyde is reduced.
“That’s what you can smell on a heavy drinker’s breath the morning after the night before,” he said. “High acetaldehyde levels in heavy, steady drinkers is increasingly implicated in causing cancer.”
To add insult to injury, we’re just not fit as we once were. “More body fat and less muscle make the alcohol we consume more concentrated in the body, leading to dehydration and worsening the dreaded hangover,” Booker said.
After your mid-twenties it takes the body longer to recover from anything due to increasing levels of inflammation and chronic diseases, which your immune system and liver are busy fighting, said Dr Campbell.
You’re also more likely to be taking prescription medication as you get older. “These medicines can alter the way your body breaks down alcohol, leaving you with a worse hangover,” he said
Booker recommends drinking more water before, during and after boozing to limit the effects of alcohol as we age. But of course, the only way to truly avoid a hangover (and the long term damaging impacts of alcohol) is to cut your intake altogether.